Hip Abduction / ER Assessment
Hip Abduction / ER Assessment
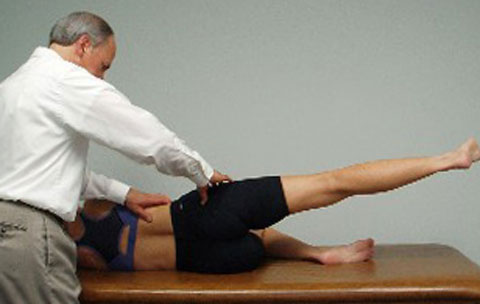
Hip abduction in supine lying with the hips and knees flexed has been commonly given to patients to help strengthen their abdominals while minimizing loading of the low back. Patients have typically been instructed to either flatten their low back while doing this exercise or to find and maintain a neutral lumbar spine during this movement. Most patients are simply instructed to flatten and then extend the low back and find the midpoint in between to obtain what they think is a neutral lumbar spine. Historically, therapists have not paid attention to the stability of the pelvis during this exercise. Mark found that when he placed his thumbs under both ASISs before the start of this exercise that the ASISs were most often asymmetrical to begin with, noting a predominance of the R ASIS appearing inferior when compared to the L side. When this asymmetry is present before initiating the HIP ABDUCTION/ER FUNCTIONAL MOVEMENT TEST, the patient is instructed to level their ASISs by bringing the R side superiorly and then hold the ASISs level as the hips are abducted. He frequently found that patients were unable to maintain the leveling of the ASISs, with the R ASIS usually dropping inferiorly before the L side. He surmised that this is indicative of an imbalance in muscle tone between the hip adductors and the abdominals on the R side signifying a loss of pelvic stability.
Mark also noted during his initial biomechanical evaluation that these patients often presented with an inferior pube dysfunction on the R side. He surmised that if the patient was given the Hip Abduction/ER exercise without consciously maintaining leveling of the ASISs the patient was reinforcing this pelvic dysfunction. Therefore, it is essential that the therapist monitors the ASISs during the performance of this movement test and teaches the patient to limit the degree of hip abduction during retraining based upon their ability to consciously maintain leveling of the ASISs throughout the exercise.
In Rehab Links Module #5 you will learn how to specifically examine your subject using the supine Hip Abduction/ER movement test. In Rehab Links Module #6 the causes and manual treatment to address the premature movement of the pelvis during this movement test are covered in detail. This is followed by the appropriate retraining exercises in Rehab Links Module #7 that are given to patients so that they can eventually perform the Hip Abduction/ER exercise without moving through the pelvis.
Lisa Chase and Mark Bookhout launched the Rehab Links Systems online platform – a unique exercise software for medical, health and fitness professionals – to help users link manual therapy treatments with a client-specific individualized home exercise program that results in improved clinical outcomes.
Click here to view the online module series and learn more. If you have already taken an exercise course with Bookhout Seminars or Back 2 Normal Institute, Rehab Links also enables you to deepen your knowledge through membership and mentoring opportunities.