Have the patient reach forward with the right hand and grasp a solid object. From this position instruct the patient to sit back diagonally towards the right hip, elongating (stretching) the right side of the back.
The right arm may be internally rotated (thumb down) or externally rotated (thumb up). Since the latissimus dorsi is an internal rotator of the shoulder internal rotation of the arm places more stretch selectively on the quadratus muscle.
Have the patient hold the stretch position for 30 seconds and repeat 2-3 times alternating sides.
Soft Tissue Mobilization of the Posterior Hip Capsule
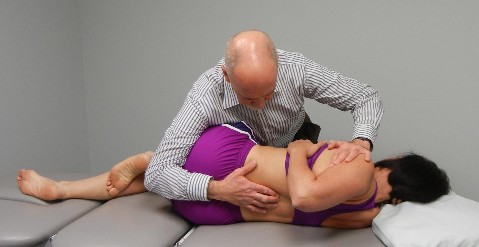
Patient is side lying with the treatment side up. The therapist uses the elbow to scour around the posterior aspect of the hip capsule feeling for areas of tension. The therapist can also work from the posterior aspect of the greater trochanter back across the gluteal area to the sacrum and address any tension in the external rotators of the hip with deep friction massage.
Passive Mobility Testing in Extension with Translation of the Shoulders from Right to Left to Detect FRS R Dysfunctions
Patient is prone propped on elbows with their elbows together and hands under their chin.
Place your right thumb on the left side of the SP and rest your left forearm over the patient’s shoulders.
Translate the patient’s shoulders from right to left as you block the SP and assess for tightness. Repeat from T10 to L3
With an FRS R dysfunction you’ll feel a blockage when attempting to draw the spine over your stabilizing L thumb
FRS dysfunctions are commonly found with this test anywhere from T11- L2 resulting in a positive FADIR test that is perceived as a tight posterior hip capsule
Patient is seated and asked to cross one leg over the other. Notice the limitation on the patient’s right side when compared to the left side. Remember that the piriformis is an internal rotator of the hip above 60 degrees of hip flexion.
Operator palpates under the twelve rib for hypertonicity in the quadratus lumborum muscle
Hypertonicity in the quadratus lumborum on one side is associated with a FRS dyfunction at the TL junction on that side, i.e., hypertonic right QL found with an FRSR at T12-L1