Dysfunctional Trunk Rotation and/or Dysfunctional Hip Abduction Functional Movement Tests
These dysfunctional movement tests can be best addressed by mobilizing any spinal dysfunctions that are found at the thoracolumbar junction and/or by stretching the quadratus lumborum and piriformis muscles. It is also sometimes helpful to mobilize the inferiomedial hip capsule and stretch the hip adductors as covered in 4b. These sources of inhibition should be addressed before attempting retraining.
Anatomy and Biomechanical Considerations:
Quadratus Lumborum, Piriformis and Posterior Hip Capsule
Observations:
Hypertonicity in the quadratus lumborum on one side is associated with a FRS dysfunction at the TL junction on that side, i.e., hypertonic right QL found with an FRS R at T12-L1.
Pinching in the anterior groin with FADIR test or when attempting to stretch the piriformis is related to a tight posterior hip capsule. “Groin pain is posterior hip capsule tightness until proven otherwise”, Dr. Philip Greenman.
An apparent tightness in the posterior hip capsule dissipates, often times dramatically, after mobilizing the upper lumbar spine for FRS dysfunctions on the same side, ie., tight R posterior hip capsule, FRS R at L1,2 or L2,3 will be present.
Therefore, before we treat the quadratus lumborum, piriformis and posterior hip capsule we need to first identify and treat any FRS dysfunctions found between T12-L2.
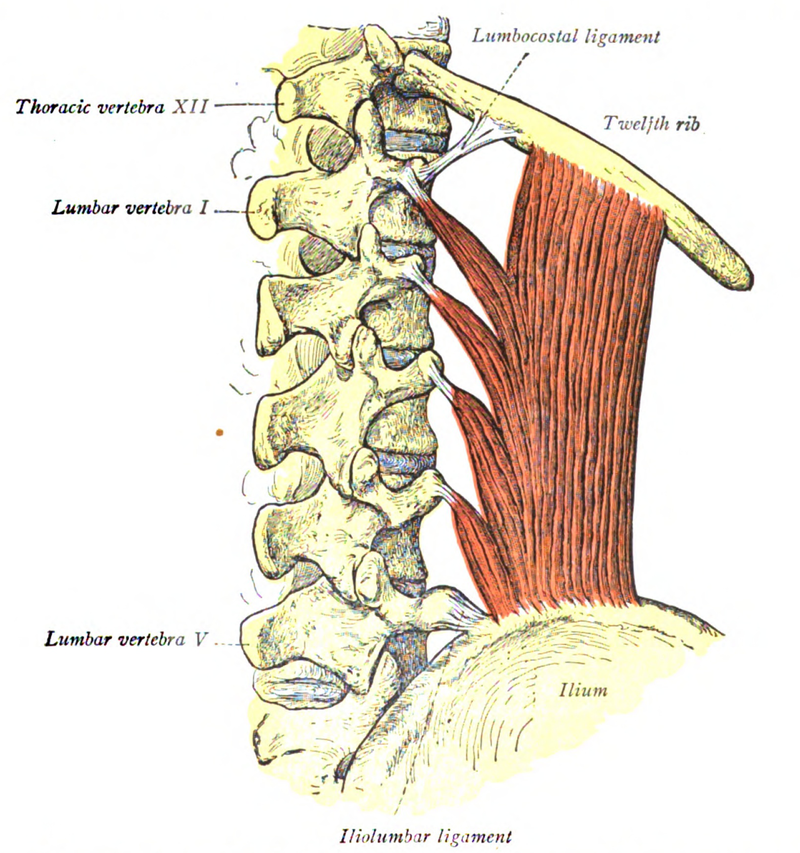
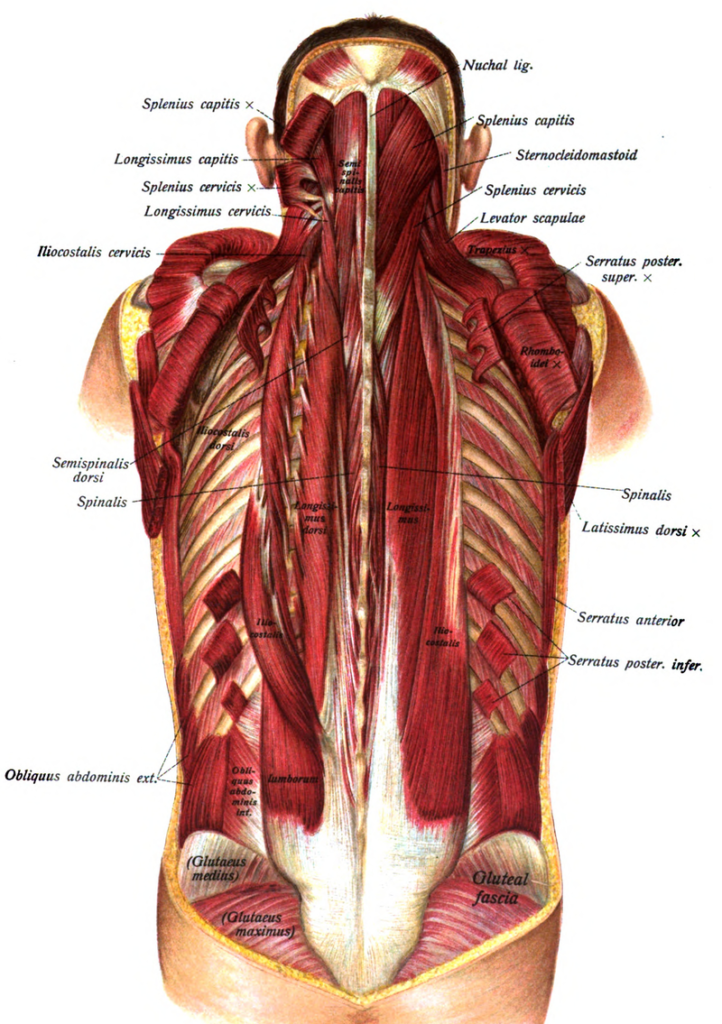
Quadratus Lumborum
Three distinct divisions:
Lateral (global mobilizer)
Iliolumbar
Lumbocostal
Function – stabilizer of the lumbar supine, a lateral flexor of the lumbar spine and a hip hiker
Innervation – thoraco-lumbar spinal nerves
Most frequent muscular cause of back pain (Travell and Simons, 1992)
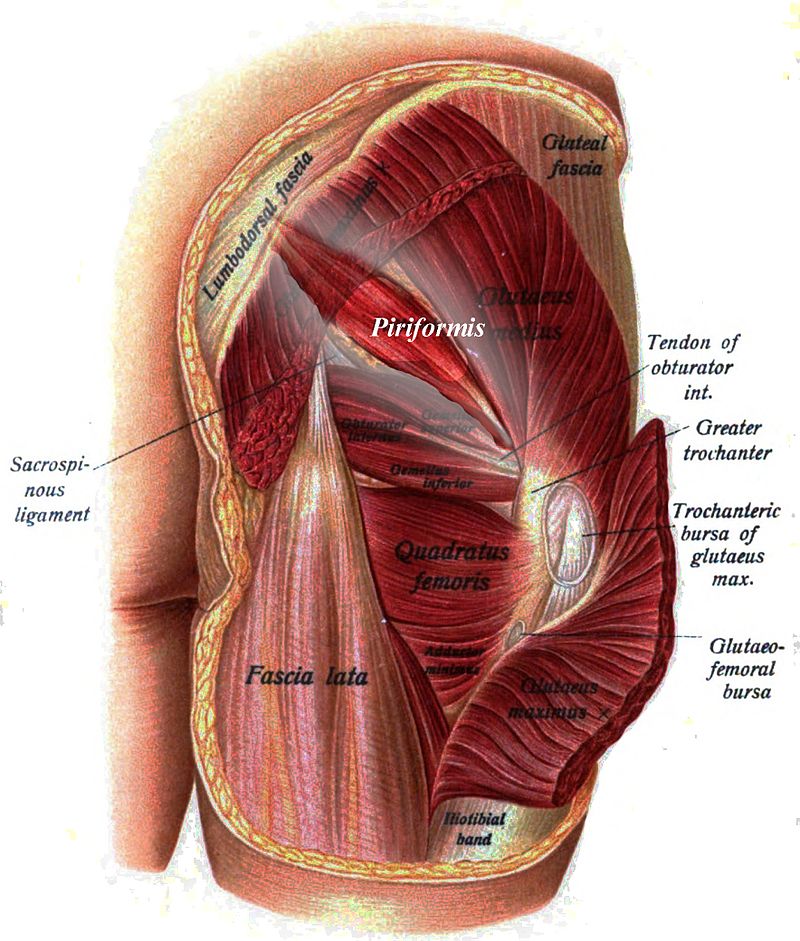
PIRIFORMIS: Origin at S 2-4, exits to insert at greater trochanter.
It crosses the SI joint and hypothetically influences the oblique axis of the sacrum during coupled motion.
Attaches to the anterior surface of S2, 3, 4 and inserts into the greater trochanter
Below 90º of hip flexion it abducts and ER the hip
Above 90º of hip flexion it abducts and IR the hip
Innervation – S1 and 2
FIVE EXTERNAL ROTATORS OF HIP Obturator internus Obturator externus Gemellus superior Gemellus inferior Quadratus femoris
(These muscles are intimately attached to the posterior hip capsule.)
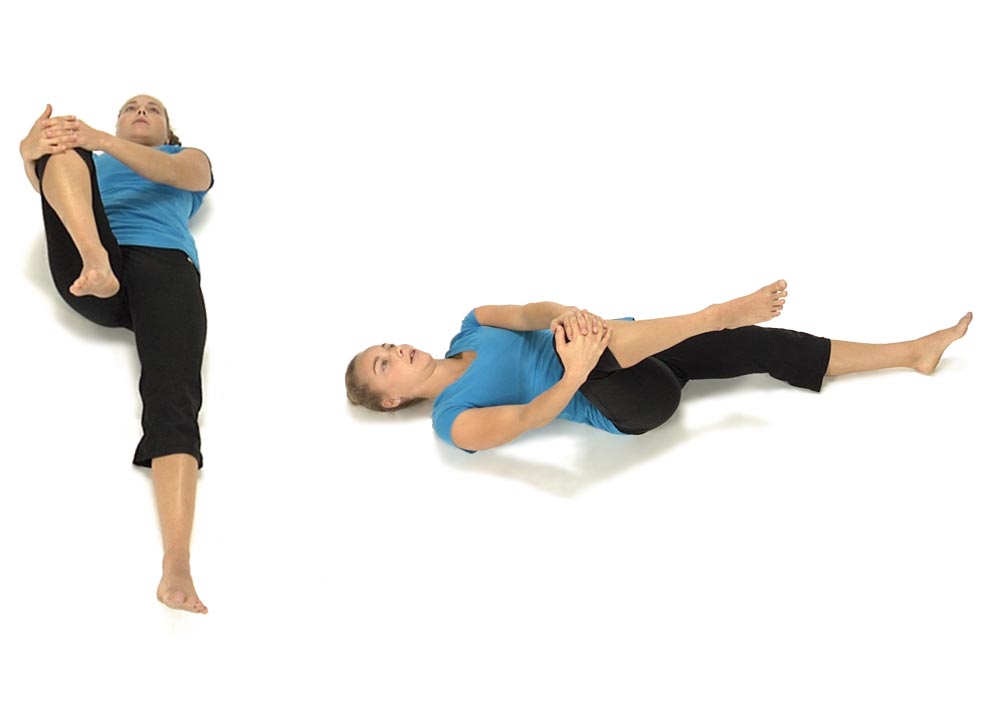
Patient is lying on their left side with a pillow under the head and the shoulder and hips perpendicular to the table.
The hips are flexed to approximately 45º with the knees flexed and the feet touching.
Ask the patient to slowly raise the right knee as high as possible keeping the feet in contact.
Compare the right to the left side, and compare any limitations noted in range of motion with the degree of inhibition of the gluteus medius on that side.
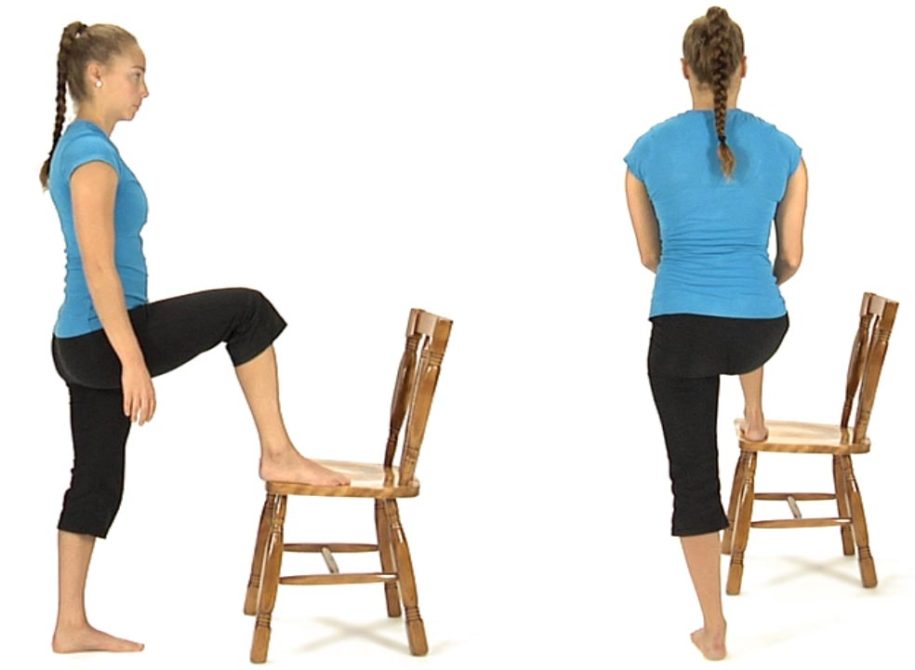
For an ERS Left and or high tone in the Left Erector Spinae:
The patient starts in standing and places their right foot up on a chair.
Instruct the patient to place their hands around each side of their right knee and slide their hands down the leg towards the ankle attempting to bring the chest down towards the right knee.
They hold the stretch for 5 to 10 seconds then return to upright standing.
Have the patient repeat this sequence 8 to 10 times.
For an ERS Right they place the left foot up on a chair.
To treat an ERS Right and/or high tone in the Right Erector Spinae:
The patient starts this exercise in the hands and knees position and is instructed to sit back diagonally as though attempting to sit onto their right hip.
Instruct the patient to sit back as far as they can without holding onto the table with their hands.
Have them hold the position for 5 seconds then come back up to the original hands and knees position without pulling up with their arms.
Muscle Energy Technique: ERS Dysfunction in the Lower Thoracic Spine
The therapist places their L index and middle fingers on the L side of the spinous processes and translates the spine towards him looking for any restriction in L to R translation (L side bending). If the restriction is worse in flexion and improves in extension the diagnosis is an ERS R.
To treat the ERS R the therapist has the patient sit up tall initially, then introduces flexion from above down and below up creating an apex for flexion at the palpated segment. L side bending is then introduced by translating the patient’s shoulders from L to R to the feather edge of the L side bending barrier. The patient is instructed to gently side bend to the R for 5-7 seconds and then relax.
The therapist takes up the slack by further translating the shoulders to the R. This is repeated 3-4 times.
Dysfunctional Supine Curl Up Functional Movement Test
This dysfunctional movement test can be best addressed by first mobilizing any ERS spinal dysfunctions that are found in the lower thoracic spine and thoracolumbar junction that restrict spinal flexion followed by stretching the erector spinae muscles. These inhibitory influences should be addressed before attempting to retrain this dysfunctional test.
It is also sometimes helpful to stretch the hip flexors as covered in #3b and c.
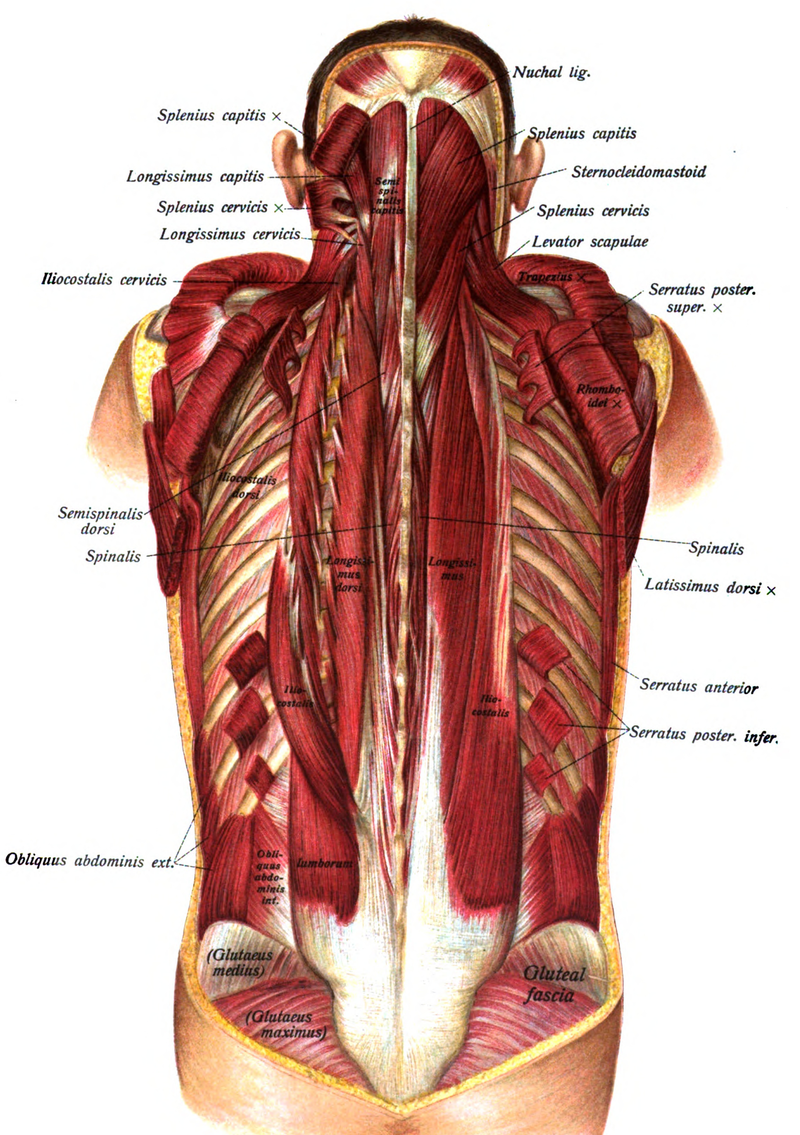
Anatomy and Biomechanical Considerations:
The erector spinae muscles consist of the longissimus thoracis and iliocostalis thoracis and iliocostalis lumborum muscles. These muscles working unilaterally rotate the spine to the ipsilateral side and when working bilaterally they extend the spine. The longissimus thoracis muscle becomes hypertonic when there is a non-neutral dysfunction in the thoracic spine. This hypertonicity, which is often seen unilaterally, results in inhibition of the abdominals and interferes with the ability to perform a curl up and/or reverse the lumbar lordosis during forward flexion.
Anterior Innominate Self Correction: Home Self-Mobilizing Exercise
Anterior Innominate Self Correction
To correct an Anterior Innominate on the right:
The patient is lying on their back keeping the left leg out straight. Using both hands they bring their R knee up towards their chest then out towards their right shoulder.
Instruct the patient to hold the right leg firmly and do not allow the leg to move as they attempt to straighten the right hip. They hold the contraction for 4-5 seconds.
When they relax instruct the patient to bring the right leg further up and out towards the R shoulder and repeat 3 to 4 times.
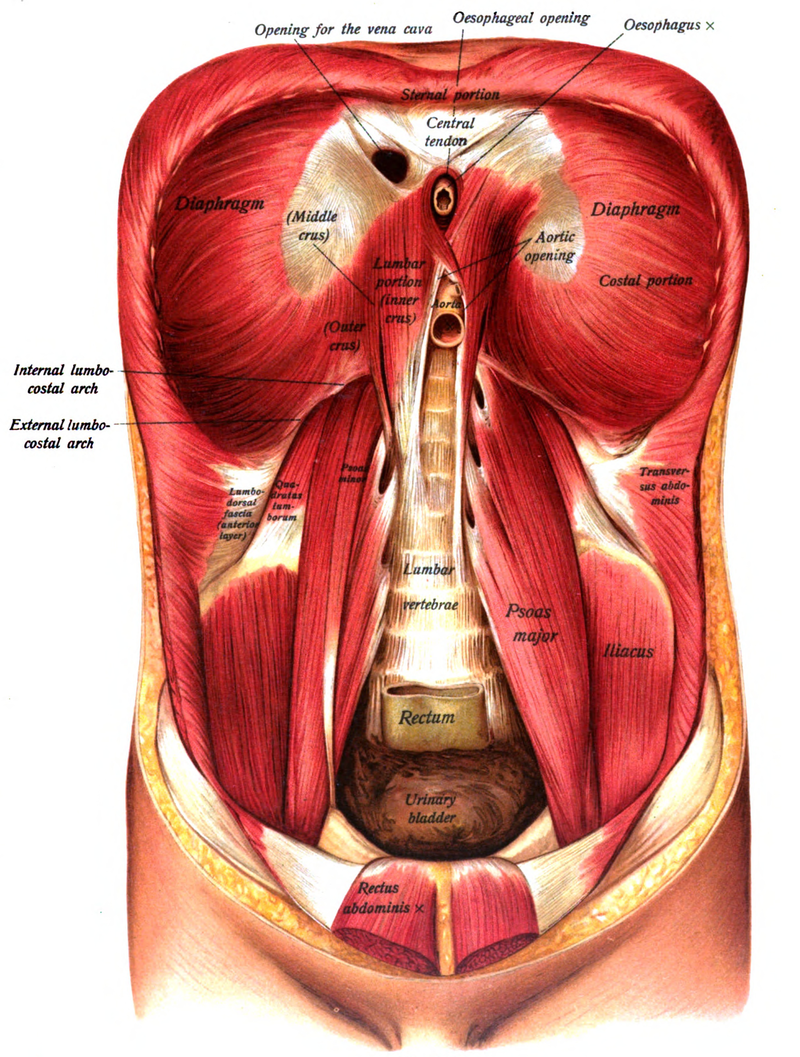
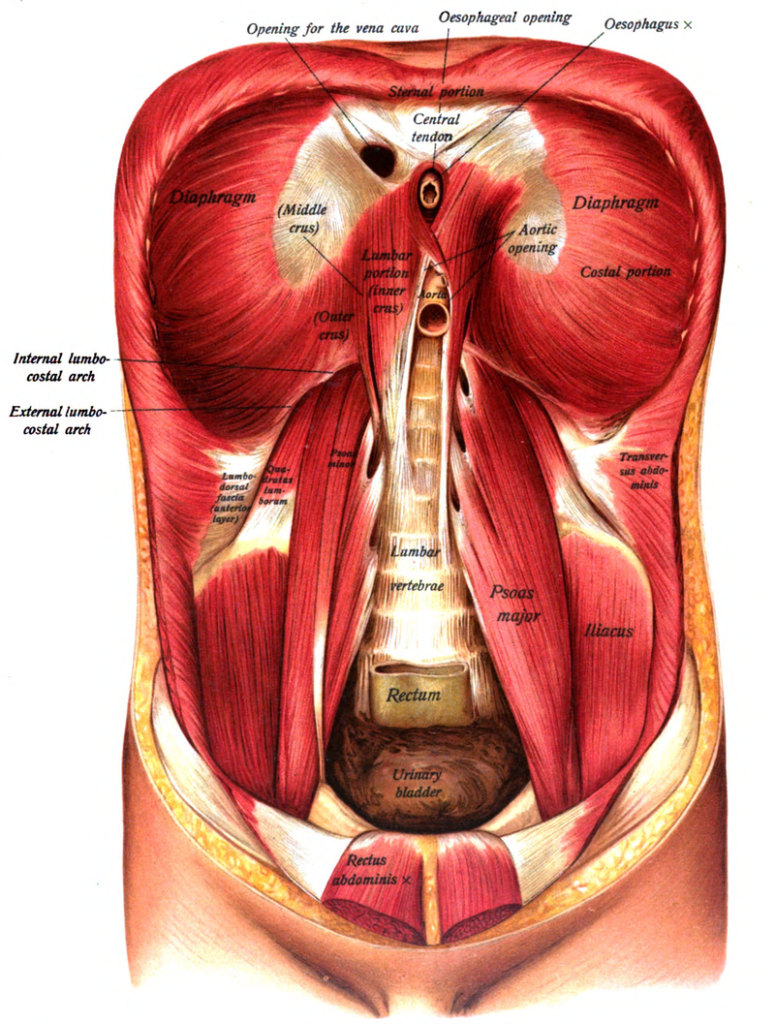
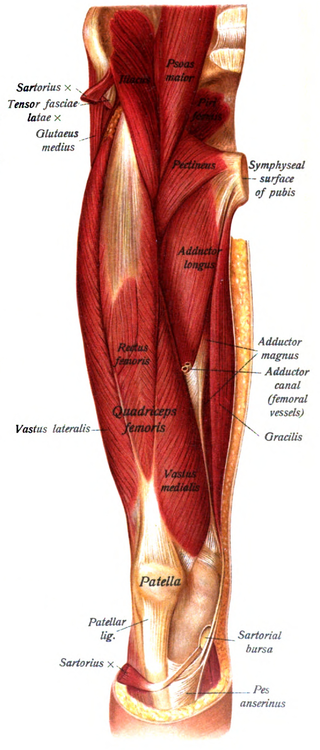
Psoas attaches to the transverse processes and vertebral bodies from T12 to L5 Iliacus attaches to the iliac fossa and sometimes anterior sacral base Powerful hip flexor and slight ER of the hip, side bends the LS to the same side and rotates away, when hypertonic these muscles limit hip extension Innervation: Femoral nerve – L2, 3 and 4
Tensor Fascia Latae:
Attached at the anterior iliac crest and ASIS Inserts into the IT band Flexes, abducts and internally rotates the hip, externally rotates the knee Innervation –Superior gluteal n. L4,5 and S1
Rectus Femoris:
Attached to the AIIS and the anterior hip capsule Flexes the hip and extends the knee Pain in the front of the knee cap is often a sign of a tight rectus femoris Innervation – femoral n. L2, 3, and 4