From the hands and knees position the patient is instructed to sit back diagonally toward their right hip as far as they can without holding on with the hands.
Make sure the patient elongates/lengthens the right side of the spine as they sit back.
Instruct the patient to hold for 10 seconds and repeat 3-5 times or they can alternate from one side to the other.
The patient should report that they feel their gluteal/buttocks muscles contract with this movement.
To increase ROM and gluteal recruitment instruct the patient to do the hands and knees quadratus lumborum/lat dorsi self stretch before this exercise.
Side Lying Hip Abduction with Elongation at the Wall
To strengthen the Left Gluteus Medius:
The patient is lying on their right side with their shoulders and hips up against a wall and the right knee bent with the right foot flat against the wall.
Patient places their left hand flat on the floor in front of them for support.
Keeping the left knee straight and the heel of their left foot touching the wall instruct the patient to slowly lift the leg up the wall.
To further facilitate the gluteus medius, have the patient reach away with their left leg (elongate) and turn the left knee slightly up towards the ceiling while lifting the leg.
They hold for 10 seconds and repeat 3-5 times initially.
The patient is instructed to avoid hiking their left hip up when raising the leg and to keep their left heel against the wall throughout the exercise to avoid substitution of hip flexion and IR by an overactive TFL and hip hiking by the quadratus lumborum.
Side lying hip abduction with both legs extended and not lying up against a wall was reported to produce the highest % of MVIC for the gluteus medius out of 12 exercises that are commonly prescribed for gluteal strengthening (DiStefano et al. 2009).
The patient is lying on their R side with their shoulders, hips and feet touching against a wall. The shoulders and hips are perpendicular to the table or floor and the hips and knees are flexed to 45-60 degrees.
Instruct the patient to draw in the abdomen using the transversus abdominis without holding their breath.
Ask the patient to lift the left knee toward the ceiling, keeping the feet in contact.
The instruction to the patient is to attempt to lift the leg up to touch the wall and then hold for 10 seconds.
The patient repeats the movement 3-5 times initially, then increases the number of repetitions as their strength improves.
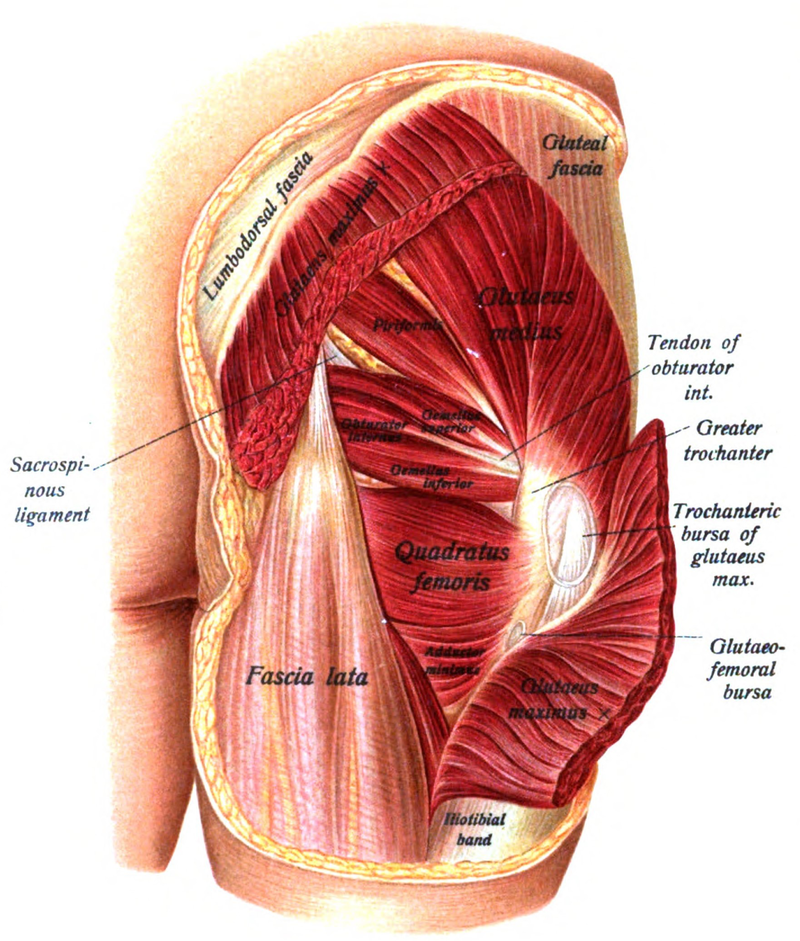
Side lying hip abduction is a test designed to assess the patient’s ability to activate the gluteus medius which is the primary stabilizer of the hip in the frontal plane. If the gluteus medius is inhibited the hip joint is subjected to long lever forces by the prime hip abductor, the tensor fascia latae (TFL). In an early degenerative hip we often see hypertonicity of the TFL and the hip adductors. If the TFL and hip adductors are hypertonic and the gluteus medius is unable to stabilize the head of the femur in the acetabulum the femoral head may be forced to migrate superiorly and laterally. This migration can result in an expulsive hip with impingement of the labrum. In addition to examining the muscle recruitment pattern in the frontal plane with this test we also test hip abduction range of motion by asking the patient to raise the knee in side lying with hip abduction/external rotation (clam). In addition to giving us information about hip joint mobility this movement test is more selective for activation of the posterior fibers of the gluteus medius and superior gluteus maximus with reduced participation of the TFL (Selkowitz, Beneck, Powers, 2013).
Innervation – Superior gluteal nerve; L4, 5 and S1
FRS dysfunctions at L4,5 or L5,S1 can result in inhibition of the gluteals
Substitution patterns to watch out for during retraining:
When the gluteus medius is inhibited, especially the posterior fibers, the patient will overutilize the TFL resulting in hip flexion and IR during the performance of this test. Therefore the therapist should watch for any deviation of the leg from the frontal plane during retraining of the gluteus medius by instructing the patient to keep the leg as straight as possible. The patient may also hike the hip up due to overutilization of the quadratus lumborum. Instructing the patient to elongate and slightly ER the leg as they perform side lying hip abduction helps to nullify these substitution patterns.
Retraining Exercises for the Gluteus Medius (from easiest to the most difficult
Ebert et al., 2017 did an extensive literature review of 33 exercises that have been traditionally given for strengthening the gluteus medius ranking them based upon the % of MVIC generated for each exercise to help give guidance in prescribing the appropriate exercise for a patient based upon their health status and the integrity of the gluteal muscles, ie., gluteal atrophy, post-surgical, OA of the hip, etc.
Jeong et al., 2015 investigated the effect of combining gluteal strengthening with lumbar segmental stabilization exercises versus retraining with lumbar stabilization exercises alone in a group of chronic low back pain patients. They reported that although both groups benefited the group that received the combination of gluteal strengthening with lumbar segmental stabilization exercises had a greater decrease in the low back disability index, and a greater increase in lumbar muscle strength and improvement in balance.
The patient is lying supine and crosses the right leg over the left.
Instruct the patient to drop both legs to the right.
Have the patient push their knees together for 5 to 7 seconds and then relax. Upon relaxation the right leg pulls the left leg further over to the right to increase the stretch.
Repeat 3-4 times progressively.
Goal – try to touch the inside of the left knee to the floor without raising the left shoulder off the floor.
Have the patient reach forward with the right hand and grasp a solid object. From this position instruct the patient to sit back diagonally towards the right hip, elongating (stretching) the right side of the back.
The right arm may be internally rotated (thumb down) or externally rotated (thumb up). Since the latissimus dorsi is an internal rotator of the shoulder internal rotation of the arm places more stretch selectively on the quadratus muscle.
Have the patient hold the stretch position for 30 seconds and repeat 2-3 times alternating sides.
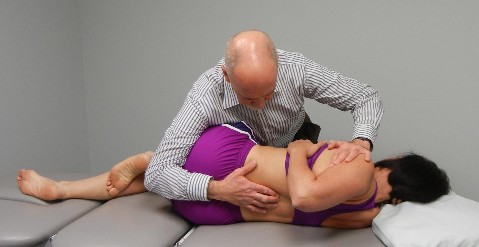
Passive Mobility Testing in Extension with Translation of the Shoulders from Right to Left to Detect FRS R Dysfunctions
Patient is prone propped on elbows with their elbows together and hands under their chin.
Place your right thumb on the left side of the SP and rest your left forearm over the patient’s shoulders.
Translate the patient’s shoulders from right to left as you block the SP and assess for tightness. Repeat from T10 to L3
With an FRS R dysfunction you’ll feel a blockage when attempting to draw the spine over your stabilizing L thumb
FRS dysfunctions are commonly found with this test anywhere from T11- L2 resulting in a positive FADIR test that is perceived as a tight posterior hip capsule