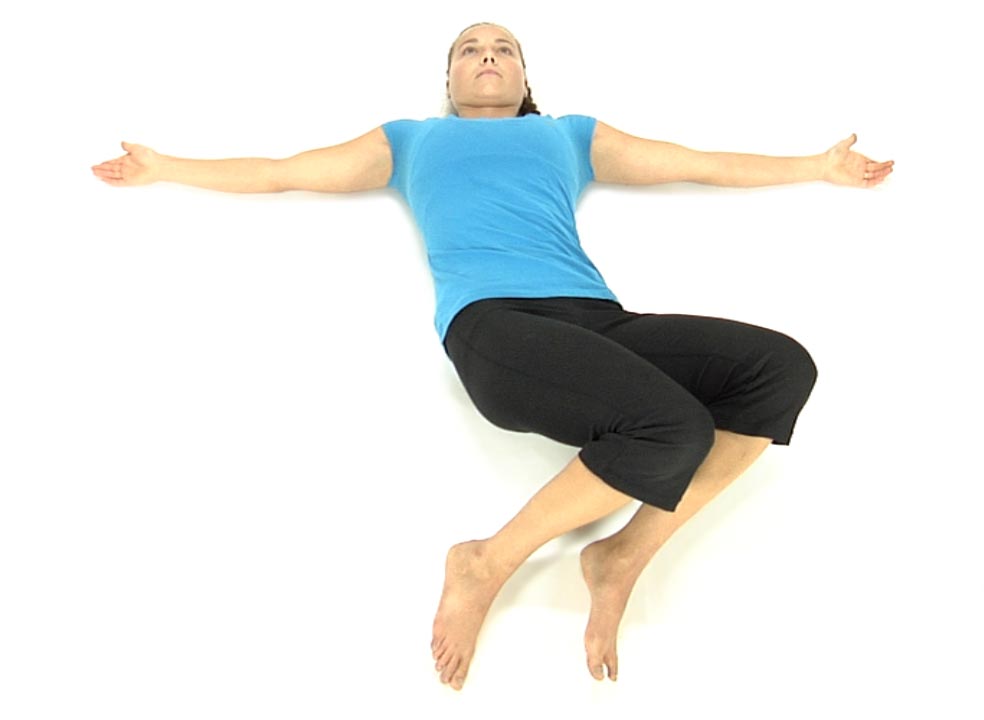
The patient is lying on their back with the knees and hips flexed and feet flat on the floor.
They are instructed to slowly drop their knees to the right approximately half way to the floor.
Ask the patient to slowly bring the knees back to the midline by flattening their back working from above down segmentally without engaging their hips, ie., T12, L1 then L2, etc. (Tell the patient to think about moving the pelvis towards 1 and 2 o’clock).
Once they’ve returned to the midline have the patient drop their knees slowly to the left, about half way to the floor.
Ask the patient to slowly bring the knees back to the midline by flattening their back working from above down segmentally without engaging their hips (Tell the patient to think about moving the pelvis towards 10 and 11 o’clock).
The patient repeats these movements alternating back and forth 3-5 times initially, gradually working up to 10 reps as their control/strength improves.
Make sure that the patient does not initiate the return to midline movement through the hips, but rather through the spine.
Active trunk rotation occurs by the combined activation of the abdominal obliques, multifidi and the erector spinae muscles. This functional movement test also requires that the patient has normal and symmetrical facet joint mobility for flexion and rotation in the lower thoracic and lumbar spines. Restricted spinal rotation, secondary to non-neutral segmental dysfunctions, especially an ERS dysfunction from T6 to L2 that limits segmental flexion and rotation, can interfere with the performance of this test. Consequently ERS dysfunctions found from T6 to L2 need to be addressed as described in module #3. before attempting to retrain this dysfunctional movement pattern with the following exercise.
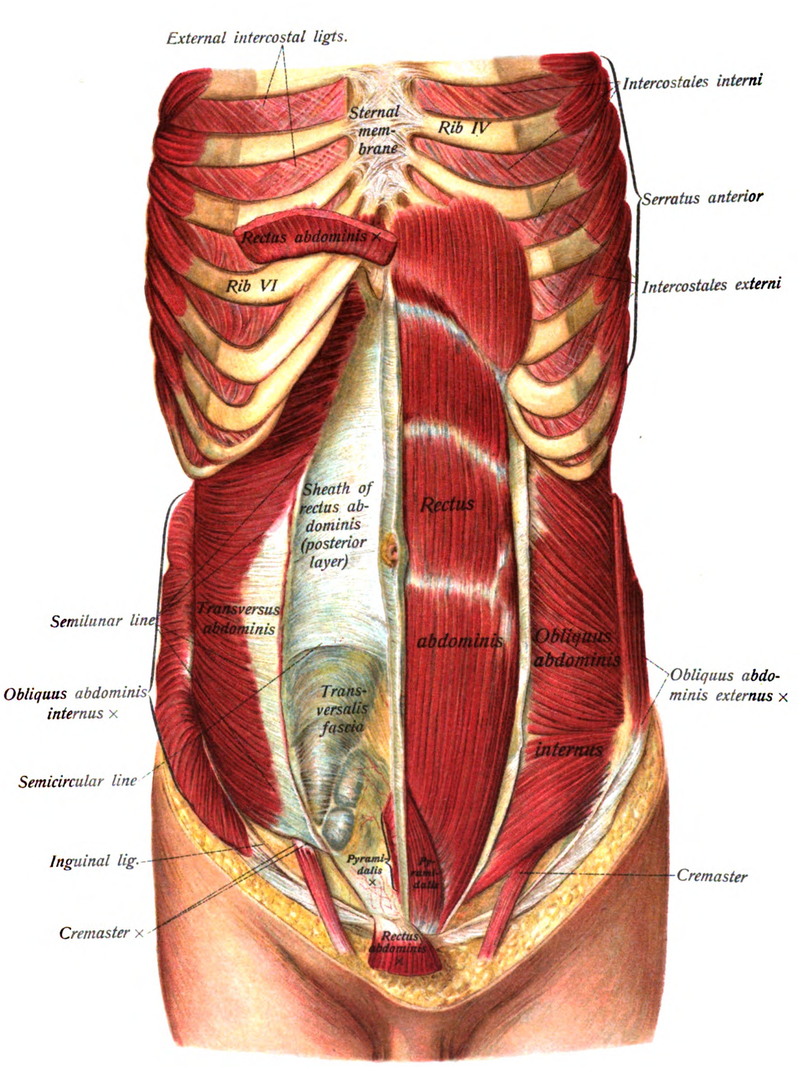
Abdominal Obliques: Key Global Mobilizers for rotation of the thoracic and lumbar spine and pelvis.
External Obliques – Anterior fibers attach from ribs 5 thru 8 and interdigitate with the serratus anterior. They insert into the linea alba through a broad flat aponeurosis. The lateral fibers attach from ribs 9 thru 12 and interdigitate with the latissimus dorsi. They form the inguinal ligament running from the ASIS to the pubic tubercle. Acting bilaterally they flex the lumbar spine and posteriorly tilt the pelvis. Acting unilaterally they laterally flex the spine to the same side and rotate away, similar to the action of the SCMs.
Innervation – T5 to T12 intercostal nerves
Internal Obliques – Anterior fibers attach along the lateral two-thirds of the inguinal ligament and iliac crest and insert into the crest of the pubis and linea alba. The lateral fibers attach to the middle third of the iliac crest and thoracolumbar fascia and insert to the inferior borders of ribs 10-12. Acting bilaterally they flex and posteriorly rotate the pelvis. Acting unilaterally with the anterior fibers of the external obliques on the opposite side they rotate the thorax forward, when the pelvis is fixed, or rotate the pelvis backward when the thorax is fixed.
Innervation – T7-12 intercostal nerves, iliohypogastric and ilioinguinal nerves
The oblique abdominals also have a vertical component to their orientation meaning that when they contract they also cause simultaneous flexion of the trunk and therefore the lumbar spine. The role of the multifidus in rotation is to oppose this flexion effect and not by themselves do they produce rotation of the spine (Bogduk and Twomey, 1991).
Substitution Patterns to watch out for during retraining:
Patients will often substitute by using the hip external rotators to bring the legs and pelvis back to the table rather than using the obliques when performing this test. Therefore the therapist should instruct the patient to initiate and perform this movement from the trunk and not from the hips. We propose that hypertonicity and chronic tightness of the hip external rotators, especially the piriformis, may be due to this dysfunctional motor control substitution pattern.
Patients will often substitute by overutilization not only of the hip external rotators, but also by using the quadratus lumborum or the lateral fibers of the obliques resulting in frontal plane side bending. They may also substitute for the multifidus by using the erector spinae muscles resulting in excessive segmental extension to compensate for the lack of control in the transverse plane. Therefore the therapist should watch for any trunk side bending or spinal extension that may occur when retraining the patient in the performance of the following exercise. Not only can these substitution patterns be palpated with your fingers placed alongside the spinous processes as demonstrated in module #2, but an astute therapist can often observe these substitution patterns as they occur by asking the patient to slowly and repeatedly rotate the legs and pelvis back and forth from side to side.
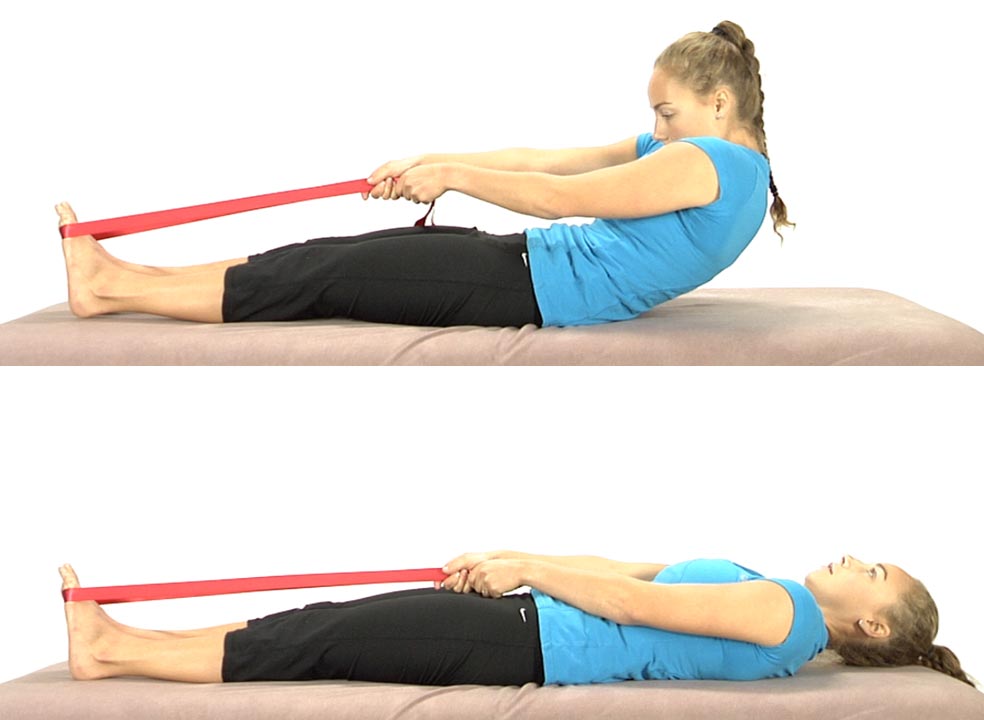
The patient starts in the long sitting position with a belt wrapped around the balls of the feet.
Instruct the patient to slowly slump back as though trying to touch their spine to the table segmentally from below up (S1, then L5, L4 etc.).
Emphasis is placed on posterior translation at each segmental level.
They’re only allowed to roll back as far as they can while maintaining spinal flexion.
Once they are able to control segmental flexion eccentrically then they can roll all the way back to the table and then come back up using the belt to assist as needed.
Have the patient repeat the exercise 8 to 10 times trying to work a little further back each time.
Goal – Eventually the patient should be able to roll all the way back and curl back up with segmental flexion without needing to use a belt to assist and without extending the spine while curling up.
Belt Assisted Eccentric Curl Backs with Therapist Assist
The patient starts sitting upright with a belt wrapped around the balls of the feet.
The patient is instructed to slowly slump back as though they are trying to touch their spine to the table segmentally from below up (S1, then L5, L4 etc.).
The therapist uses manual contacts to the abdominals and also to the spine to bring sensory awareness to specific levels of the spine as the patient proceeds.
Emphasis is placed on posterior translation at each segmental level.
The patient is only allowed to roll back as far as they can while maintaining spinal flexion.
Once they can control segmental flexion eccentrically then they can roll all the way back to the table and then come back up using the belt to assist as needed.
The inability to perform a supine curl up is often due to an ERS dysfunction in the lower thoracic spine or upper lumbar spine and should always be addressed first before attempting to retrain this movement test. (Refer to Module #3). When patients perform abdominal “crunches” with the hips and knees flexed they are working the abdominals in a shortened position and often results in substitution by the hip flexors. We need to consider that working the abdominals with the hips and knees flexed is not really functional as we need abdominal tension/tone through the full range of flexion of our spine. This is especially true when we are standing upright with the hips and knees in a neutral or extended position. Often what we see in the clinic are people who are unable to perform an unassisted full range supine curl up without extending the lumbar spine when the hip flexors kick in at mid range.
Working the abdominals eccentrically with the assistance of a belt helps to not only activate the abdominals throughout the full spinal flexion range of motion, but also can be used to segmentally self mobilize the thoracolumbar spine for flexion. In addition, this exercise stretches the thoracolumbar spinal extensors that are prone to hypertonicity as a response to abnormal afferent information in the lower quarter. We see this especially in patients complaining of low back pain.
When working the abdominals eccentrically, emphasis is placed on instructing the patient to posteriorly translate the spine segmentally from below up and to stop when they reach a spinal level that they are unable to flex (posteriorly translate). This exercise is therefore ideal for patients with spondylolisthesis who need to strengthen their abdominals and avoid exercises that can cause or contribute to anterior translation of L5 or L4. This exercise is also helpful for patients with lumbar central and lateral stenosis as spinal flexion increases spinal canal volume and opens the intervertebral foramen respectively.
Substitution Patterns to watch out for during retraining:
When instructing a patient in this exercise focus on encouraging the patient to draw the belly in and push their spine back to maximally posteriorly translate the spine at each spinal level beginning at L5 and working segmentally up the spine. Look for a loss of flexion at a spinal level when there is a tendency to extend rather than flex through this level. When this occurs the patient should be instructed to return upright by curling back up to the starting position and repeat the exercise. The patient should be able to gradually lower themselves further and further until eventually they are able to touch the floor.
The patient is lying on the back, with their thumbs placed above the ASISs to monitor pelvic stability.
The patient is instructed to find the midpoint between 12:00 and 6:00 o’clock then draw the belly in towards the spine without flattening the low back so that they maintain a neutral lumbar spine.
The patient continues to monitor the position of the ASISs as they slowly drop the right knee out to the side.
The patient is instructed that if the R ASIS drops inferiorly when compared to the L ASIS while abducting and externally rotating the R hip they are to return back to the midline and start over.
The patient is instructed not to drop the R knee out to the side further than they can maintain leveling at the ASISs.
Repeat on both sides for 3-5 repetitions to start, increasing to 10 reps.
Bilateral Hip Abduction and External Rotation with a Neutral Lumbar Spine
The patient is lying on their back and instructed to find neutral, midway between 12:00 and 6:00 while monitoring the ASISs with their thumbs.
Instruct the patient to maintain neutral and draw the belly in towards the spine without flattening the low back.
While monitoring the ASISs with their thumbs ask the patient to slowly separate the knees while keeping the ASISs still/level.
If either ASIS begins to move inferiorly (towards the feet) instruct the patient to stop and bring the knees back to the midline and start over.
Repeat 3-5 times
The goal is for the patient to be able to maintain a neutral lumbar spine and symmetrically abduct and externally rotate both hips without either ASIS moving inferiorly.
Dysfunctional Supine Abduction and External Rotation Test
Anatomy and Biomechanics:
The pubic symphysis is a fibrocartilagenous joint whose stability is dependent upon a balance of tension/tone between the superior muscle attachments (obliques and rectus abdominis) and the inferior muscle attachments (hip adductors). Pubic dysfunctions are a reflection of an imbalance in tension between these two competing muscle groups. Abdominal surgeries, ie, appendectomies, hernia repairs, c-sections all result in scarring and fibrosis of the abdominals resulting in inhibition of the abdominals and contribute to the development of an inferior pubic shear. An inferior pubic shear occurs due to the dominance of the hip adductors that respond to abnormal afferent information by becoming hypertonic. This is more commonly seen on the right side. Rebalancing these competing muscle groups is a goal for the following home exercises.
Substitution Patterns to watch out for during retraining:
Dysfunction with this movement test is almost always found on the right versus the left side so pay attention to the R ASIS which will drop inferiorly prematurely when compared to the left side. Tightness of the R medial and anterior hip capsule, hypertonicity of the R hip adductors and an inferior pubic shear dysfunction on the R side can all result in a positive test and need to be addressed before retraining is initiated.
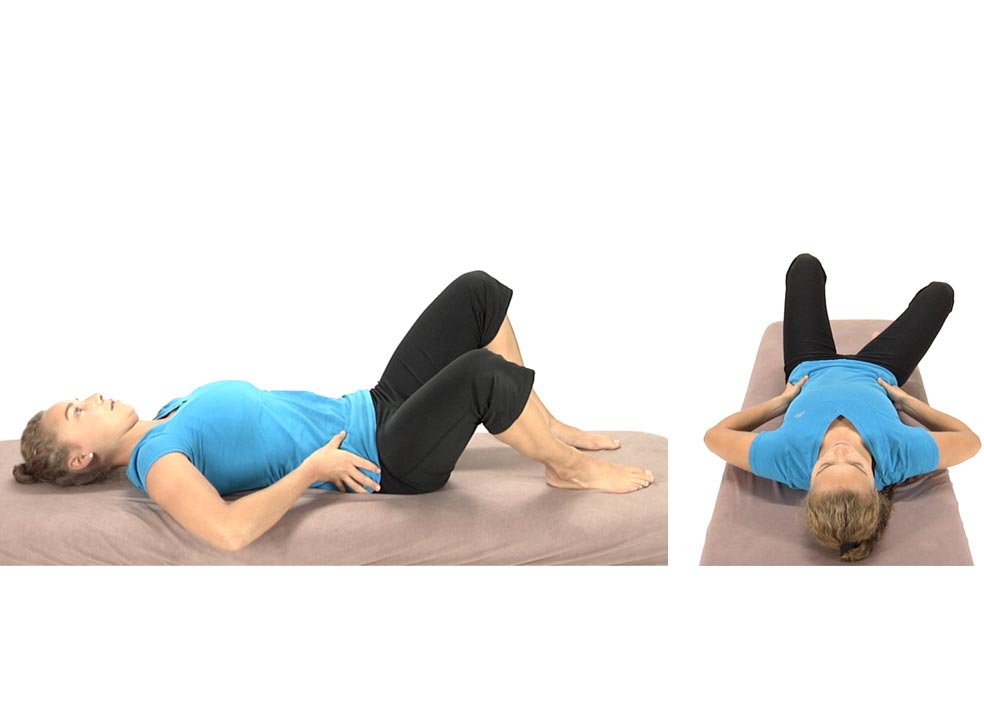
The patient is lying on their back with both hips flexed to approximately 90º. Ask the patient to find a neutral lumbar spine by having them roll the pelvis from 12 to 6 and find the midpoint.
The patient monitors the ASISs with their thumbs to keep them level.
Instruct the patient to slowly touch one heel to the table, alternating between the right and left sides while monitoring the ASISs and not allowing an ASIS to drop inferiorly on either side.
As their strength improves, they can start extending the hip out further to touch the heel (bottom picture).
Have them repeat 3-5 times and increase repetitions as their strength improves.
The patient is lying supine with their hips and knees flexed and the feet flat on the table.
Instruct the patient to find a neutral lumbar spine position, midway between 12:00 and 6:00, monitoring the ASISs with their thumbs.
Have the patient draw their belly in without flattening the low back (the ASISs should not move when they draw the belly in).
Instruct the patient to slowly slide their right heel along the table while monitoring the ASISs. The right ASIS should remain stable as the right leg is extended. If the ASIS moves inferiorly, the patient should stop, and bring the leg back up to the starting position.
Goal – the patient should be able to fully straighten either leg without the ASISs moving while maintaining a neutral lumbar spine.
They repeat the exercise 3-5 times initially and increase repetitions as their performance improves.