Bilateral Hip Abduction and External Rotation with a Neutral Lumbar Spine
The patient is lying on their back and instructed to find neutral, midway between 12:00 and 6:00 while monitoring the ASISs with their thumbs.
Instruct the patient to maintain neutral and draw the belly in towards the spine without flattening the low back.
While monitoring the ASISs with their thumbs ask the patient to slowly separate the knees while keeping the ASISs still/level.
If either ASIS begins to move inferiorly (towards the feet) instruct the patient to stop and bring the knees back to the midline and start over.
Repeat 3-5 times
The goal is for the patient to be able to maintain a neutral lumbar spine and symmetrically abduct and externally rotate both hips without either ASIS moving inferiorly.
Dysfunctional Supine Abduction and External Rotation Test
Anatomy and Biomechanics:
The pubic symphysis is a fibrocartilagenous joint whose stability is dependent upon a balance of tension/tone between the superior muscle attachments (obliques and rectus abdominis) and the inferior muscle attachments (hip adductors). Pubic dysfunctions are a reflection of an imbalance in tension between these two competing muscle groups. Abdominal surgeries, ie, appendectomies, hernia repairs, c-sections all result in scarring and fibrosis of the abdominals resulting in inhibition of the abdominals and contribute to the development of an inferior pubic shear. An inferior pubic shear occurs due to the dominance of the hip adductors that respond to abnormal afferent information by becoming hypertonic. This is more commonly seen on the right side. Rebalancing these competing muscle groups is a goal for the following home exercises.
Substitution Patterns to watch out for during retraining:
Dysfunction with this movement test is almost always found on the right versus the left side so pay attention to the R ASIS which will drop inferiorly prematurely when compared to the left side. Tightness of the R medial and anterior hip capsule, hypertonicity of the R hip adductors and an inferior pubic shear dysfunction on the R side can all result in a positive test and need to be addressed before retraining is initiated.
The patient is lying on their back with the hips and knees flexed and feet flat on the table.
Have the patient place their hands on both sides of the lower rib cage.
Ask the patient to find a neutral lumbar spine by rolling the pelvis towards 6 and 12 o’clock and finding the midpoint in the range.
Instruct the patient to draw the belly in without flattening their lower back maintaining a neutral lumbar spine. The patient monitors the ASISs to make sure that they remain level throughout this exercise.
Instruct the patient to slowly inhale through the nose allowing their lungs to fill with air as the rib cage expands out to the sides as they draw the navel in. Their chest and shoulders should remain relaxed and they should not feel that their belly pushes out or that the lower ribs are pulled down and medially by the obliques which can often substitute with transversus abdominis dysfunction.
The patient exhales through pursed lips and allows the ribs to fall down and in. Their upper chest should continue to remain relaxed.
If they are having difficulty recruiting the transversus have them blow out as much air as possible during exhalation using their abdominal muscles to assist and hold for 3-5 seconds. Then have them slowly inhale while continuing to draw the belly in and hold for 10 seconds.
Have them repeat up to 10 times holding for 10 seconds each time.
The patient is lying on their back with the hips and knees flexed and feet flat on the table.
Have the patient place their hands on both sides of the lower rib cage.
Instruct the patient to slowly inhale through the nose allowing their lungs to fill with air as the rib cage expands out to the sides as they draw the navel in. Their chest and shoulders should remain relaxed and they should not feel that their belly pushes out or that the lower ribs are pulled down and medially by the obliques which can often substitute for transversus dysfunction.
The patient exhales through pursed lips and allows the ribs to fall down and in. Their upper chest should continue to remain relaxed.
Have them repeat up to 10 times holding for 10 seconds each time.
Starting in hands and knees with the hips positioned directly over the knees and the shoulders positioned directly over the hands, the patient is instructed to bend their elbows so that the shoulders are the same height as the hips.
The patient is instructed to find a neutral lumbar spine by rocking the pelvis from 12:00 to 6:00 and finding the midrange position.
The therapist monitors the PSISs to insure that they are level in the frontal plane before starting and during the performance of this exercise.
Instruct the patient to draw the belly up and in towards the spine without changing the lumbar neutral position. The therapist monitors the PSISs to insure that they remain stable and provides verbal feedback to the patient if any deviation should occur. The therapist should watch for any loss of the neutral lumbar spine position during the exercise.
Ask the patient to lift the left hand off the table and maintain a level pelvis and shoulder girdles.
Make sure the patient keeps their right elbow bent, shoulders level and they don’t drop their head when they lift their left hand.
Then have the patient switch sides lifting up the right hand.
The patient is instructed to hold for 10 seconds on each side as one repetition and repeat 3-5 times, gradually working up to 10 reps.
Starting in hands and knees with the hips positioned directly over the knees and the shoulders positioned directly over the hands, the patient is instructed to bend their elbows so that the shoulders are the same height as the hips.
The patient is instructed to find a neutral lumbar spine by rocking the pelvis from 12:00 to 6:00 and finding the midrange position.
The therapist monitors the PSISs to insure that they are level in the frontal plane before starting and during the performance of this exercise.
Instruct the patient to draw the belly up and in towards the spine without changing the lumbar neutral position. The therapist monitors the PSISs to insure that they remain stable and provides verbal feedback to the patient if any deviation should occur. The therapist should watch for any loss of the neutral lumbar spine position during the exercise.
The patient is instructed to hold for 10 seconds and repeat 3-5 times.
Muscle Energy Technique: ERS Dysfunction in the Lower Thoracic Spine
The therapist places their L index and middle fingers on the L side of the spinous processes and translates the spine towards him looking for any restriction in L to R translation (L side bending). If the restriction is worse in flexion and improves in extension the diagnosis is an ERS R.
To treat the ERS R the therapist has the patient sit up tall initially, then introduces flexion from above down and below up creating an apex for flexion at the palpated segment. L side bending is then introduced by translating the patient’s shoulders from L to R to the feather edge of the L side bending barrier. The patient is instructed to gently side bend to the R for 5-7 seconds and then relax.
The therapist takes up the slack by further translating the shoulders to the R. This is repeated 3-4 times.
Dysfunctional Hip Abduction and ER and/or Dysfunctional Hip Abduction Functional Movement Tests
These dysfunctional movement tests are best addressed by mobilizing the inferiomedial hip capsule, stretching the hip adductors and/or obturator nerve, and mobilizing the sacral base to restore restricted anterior nutation on the dysfunctional test side before retraining is initiated. Also a pubic symphysis dysfunction needs to be addressed, if present, as it represents an imbalance in tone between the hip adductors and abdominals and can contribute to, or be the source of these dysfunctional movement tests.
Mobilizing the hip in an inferiomedial direction in side lying at 45 degrees of passive hip abduction has been shown to improve isometric torque in the hip abductors, in the short term, in healthy subjects. (Makofsky et al., 2007). This response is proposed to be due to a reduction of an inhibitory and dysfunctional arthrokinetic reflex from a tight inferiomedial joint capsule (Warmerdam, 1999).
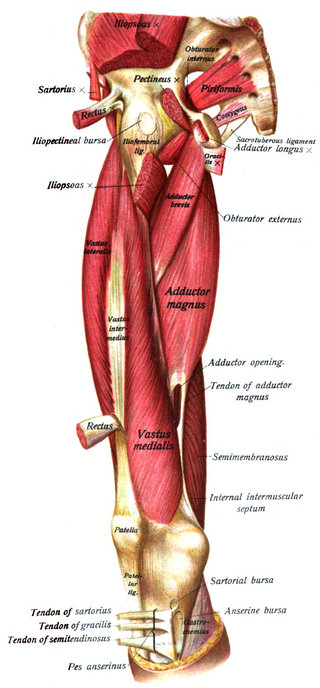
Anatomy and Biomechanical Considerations:
Hip Adductors
Attach to the pubic ramus and ischial ramus to ischial tuberosity
Function to restrain abduction of the stance limb during gait
They also assist in internal rotation and flexion of the hip
Hypertonicity of the hip adductors can result in displacement of the femoral head superiorly and laterally
Innervation – obturator n. L2, 3 and 4
Anterior Oblique Sling
Adductors are functionally connected to the abdominal obliques on the contralateral slide to form an oblique sling of support for the anterior pelvis
When hypertonic the pull of the adductors can result in an inferior pubic shear
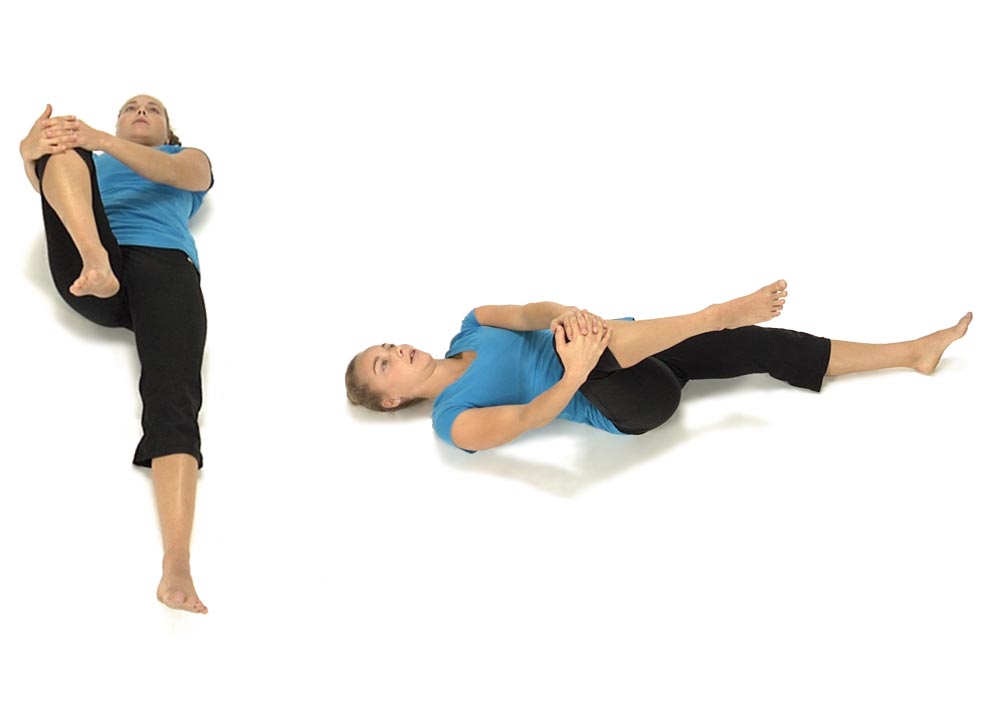
Anterior Innominate Self Correction: Home Self-Mobilizing Exercise
Anterior Innominate Self Correction
To correct an Anterior Innominate on the right:
The patient is lying on their back keeping the left leg out straight. Using both hands they bring their R knee up towards their chest then out towards their right shoulder.
Instruct the patient to hold the right leg firmly and do not allow the leg to move as they attempt to straighten the right hip. They hold the contraction for 4-5 seconds.
When they relax instruct the patient to bring the right leg further up and out towards the R shoulder and repeat 3 to 4 times.
The patient is supine and is initially positioned in the same starting position as for the pelvic clock assessment. The subject is instructed to posteriorly rotate the pelvis towards 12 o’clock which is monitored by the examiner’s thumbs placed either inferior or superior over the ASISs. The ASISs must be level in the frontal plane prior to the start of the movement test. If asymmetry at 12:00 o’clock is present the subject is usually asked to draw the right ASIS superiorly further (usually accomplished by side bending the trunk to the right). The subject is asked to maintain the symmetrical 12 o’clock position and slowly abduct, or allow the knees to separate as far as possible, without losing the symmetry at the monitored ASISs. The operator monitors the ASIS position and notes if one side begins to drop caudally as the subject slowly drops the knees out to the side.