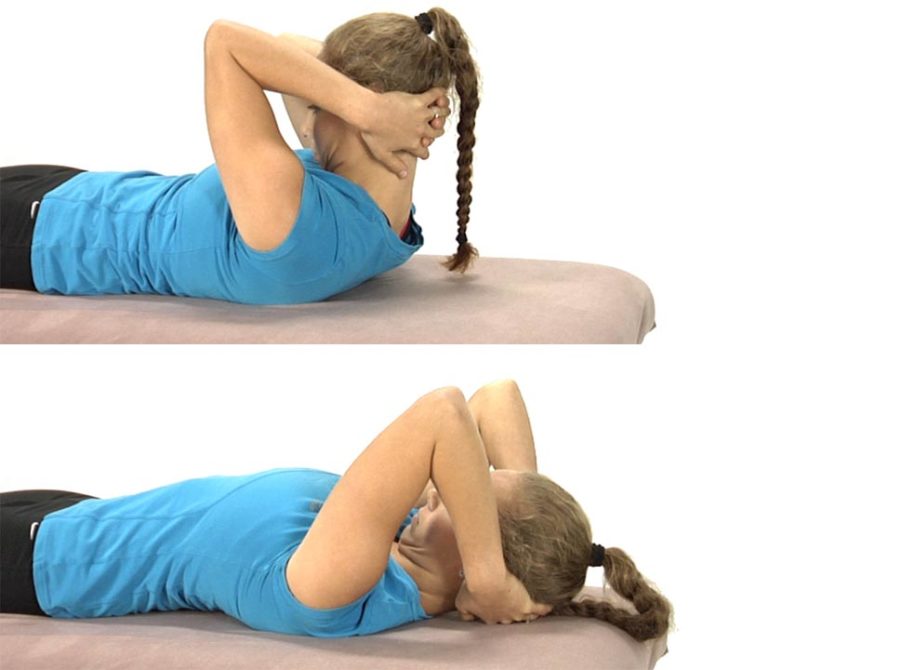
The patient is lying on their back with their hands clasped behind the head.
Instruct the patient to only use their arms to lift their head up so that the chin is drawn toward the chest and a stretch is felt through the back of the neck.
Once the head is brought up fully the patient is told to hold this position for 5-10 seconds, then slowly lower the head back to the table segmentally from below up, using the deep neck flexors eccentrically to lower the head back down to the table and assisting the movement with their hands as needed.
The hands only support the head as needed and an emphasis is placed upon keeping the chin down as the head is returned back to the table.
They repeat 3-5 times.
Eventually as the deep neck flexors become stronger, the hands should no longer be needed to assist in slowly returning the head back to the table.
The goal with this exercise is for the patient to be able to segmentally flex the neck and return back down to the table segmentally without using the hands to assist with the chin staying down throughout the entire movement.
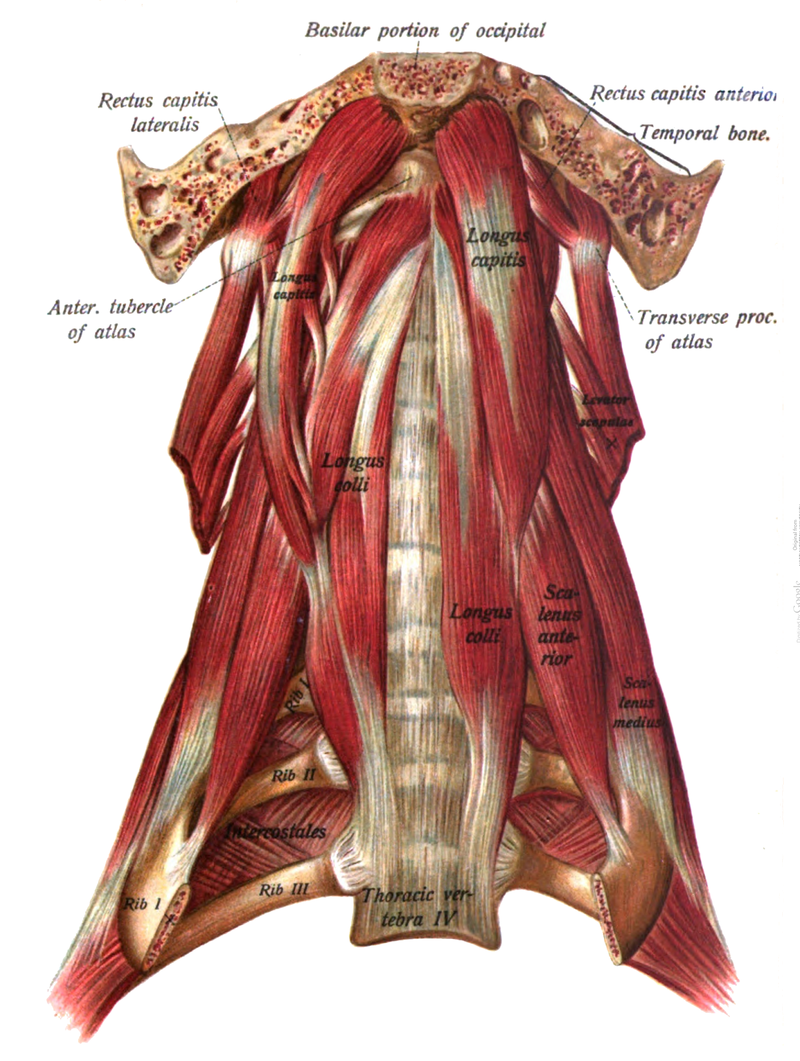
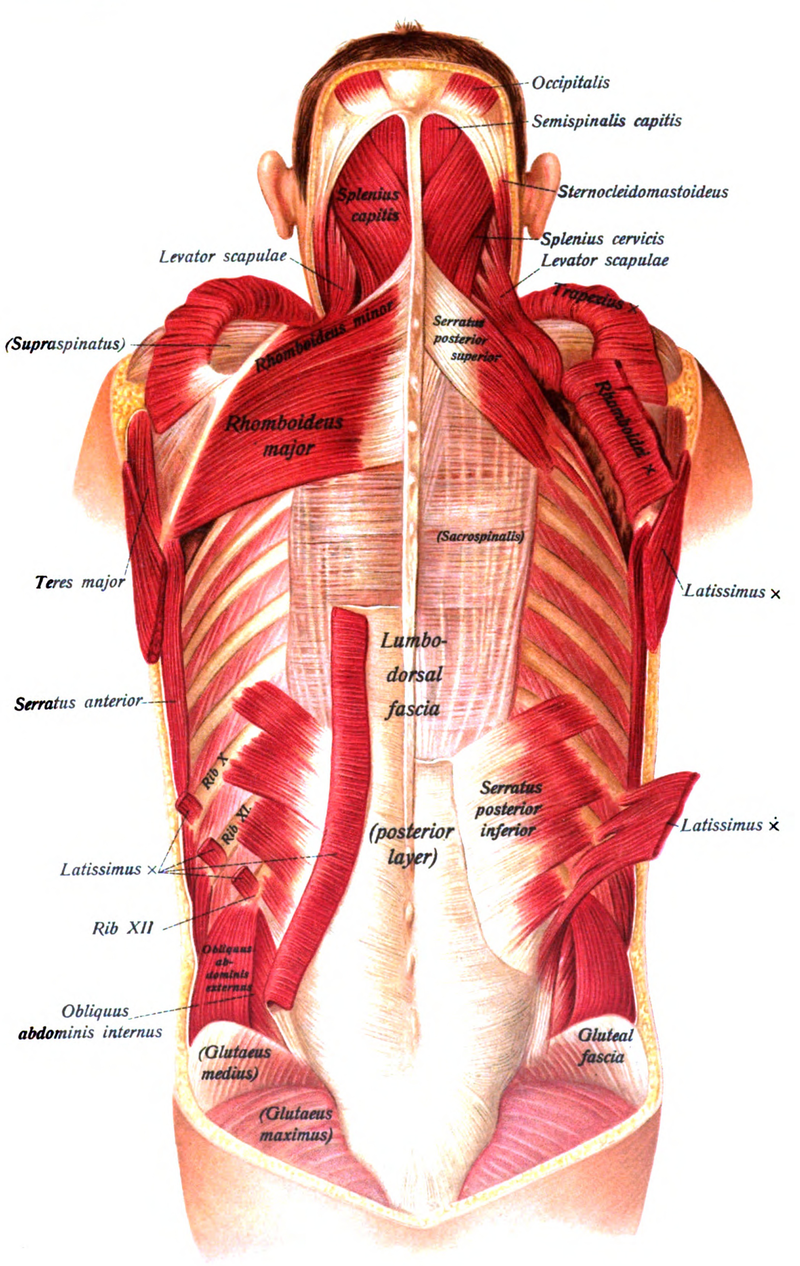
The cervical flexion test assesses the ability of the patient to segmentally flex the cervical spine using the longus colli, longus capitis and rectus capitis anterior assisted by the SCMs, anterior scalenes and infra and suprahyoid muscles. When the primary deep neck flexors are inhibited/weak the SCMs and anterior scalenes substitute for this weakness and become the primary neck flexors resulting in the chin tipping up and the upper CS extending rather than flexing during the performance of this test (Janda, 1994).
Abnormal afferent information that can contribute to this muscle imbalance can occur when ERS dysfunctions of the cervical and especially upper thoracic spine are present. These ERS dysfunctions can result in inhibition of the longus colli and longus capitis due to restricted active and passive ROM for neck flexion. In addition, hypertonicity of the scalenes occurs in apical chest wall breathers as the scalenes, which are normally only accessory muscles recruited with deep inhalation, become recruited with every breath. Palpation of the scalenes in these patients will confirm the recruitment of these muscles even during relaxed breathing. This typically is felt to occur more on the R side than the L. Asking these patients to take a deep breath while the therapist palpates the lower lateral rib cage for normal bucket handle motion will reveal restricted excursion on the R side in these patients.
Self-Stretching of the Upper Trapezius and Sternocleidomastoid
Upper Trapezius and SCM Stretch
These muscles extend the upper cervical spine, side bend toward the ipsilateral side and rotate the head to the opposite side
When tight these muscles may serve as long restrictors for mobility at C0-C1
To stretch the right upper trapezius and sternocleidomastoid:
Instruct the patient to position their head in flexion, side bending to the left and rotation to the right.
Their left hand is placed on top and around their head for support. Instruct the patient not to pull on the head with the left hand.
The right hand grasps the chair or bench behind the right hip.
The stretch is introduced by asking the patient to slowly lean forward and away and not by pulling on the head. They should feel a stretch over the top of the right shoulder and behind the ear.
Then instruct the patient to tuck the chin down (nod the chin) to add to the stretch which should be felt at the attachment behind the right ear.
Ask the patient to pull their right shoulder blade down and back to further increase the stretch.
They hold for 20 seconds and repeat 2-3 times. Have the patient alternate sides and stretch to symmetry as much as possible.
The patient is instructed to sit with the head positioned in flexion, left side bending and left rotation, as though looking down towards the left hip.
Their left hand is placed on top and around their head for support. Instruct the patient not to pull on their head with the left hand.
The right hand is placed behind the right hip and grasps the chair/bench.
Ask the patient to slowly lean forward and to the left to feel a stretch along the right side of their neck.
To facilitate a balance between the levator scapulae and ipsilateral lower trapezius, instruct the patient to pull their right shoulder down and back using the lower trapezius muscle. If done properly they should feel an additional stretch in the levator scapulae muscle.
They hold for 20 seconds and repeat 2-3 times on each side.
Barry Wyke, 1981 reported that when experiencing pain in the neck and/or low back there is facilitation of the spinal extensors and inhibition of the spinal flexors. In describing muscle imbalances found in his Upper Crossed Syndrome Janda (1994)) observed that the neck extensors are tight (SCM and suboccipitals) and the deep neck flexors are inhibited and weak.
Jull (1994 and 1997) studied the recruitment of the deep upper cervical flexors in patients with neck pain using a biofeedback cuff placed under the upper cervical spine that they used to measure the amount of pressure a patient can produce when asked to perform upper cervical flexion without recruiting the superficial neck flexors. Patients with neck pain were found to display a deficit in their ability to activate and maintain contraction of the deep neck flexors.
If the cervical flexion test is dysfunctional you first need to determine if there is also a restriction for passive cervical flexion. Restricted passive cervical spine flexion indicates a mobility problem that needs to be addressed first before attempting to retrain the deep neck flexors. Restricted passive neck flexion can be due to the presence of ERS dysfunctions in the upper thoracic and lower cervical spine, hypertonicity of the levator scapula and splenius cervicis muscles or as a consequence of adverse neural tension. Once passive supine cervical flexion mobility is free then retraining as presented in Module #7 can begin.
Anatomy and Biomechanical Considerations:
Cervical flexion requires that the cervical and upper thoracic facet joints can bilaterally open and slide superiorly freely. The cervical flexion test if done sequentially from above down requires that the chin approaches the chest and remains there through the full range of neck flexion. Remember that the SCM muscles when activated bilaterally, participate in flexion of the typical cervical spine, but extension of the upper cervical spine. It is because of this dual action of the SCMs that with inhibition of the deep neck flexors we see patients extend the upper cervical spine during the cervical flexion test leading with their chin up.
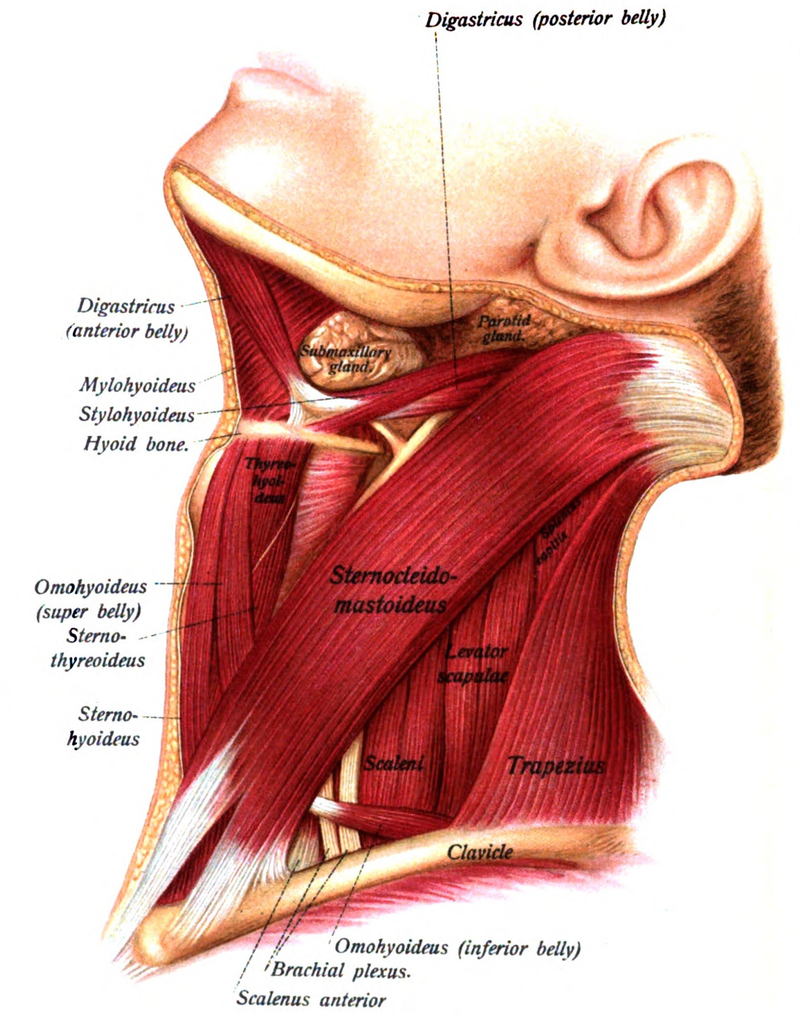
Sternocleidomastoid:
Two divisions: sternal and clavicular attach into the mastoid process of the temporal bone
Function: bilateral activation – flexion of the typical CS and extension of OA, unilateral – side bends to the same side and rotates to opposite side
Innervation – spinal accessory n., cranial XI
Levator Scapulae and Splenius Cervicis:
The levator scapulae attaches from C1-C4 and with the scapula fixed, extends, side bends and rotates the cervical spine to the ipsilateral side
When hypertonic these muscles not only restrict passive neck flexion, but also they can act as long restrictors at multiple levels of the cervical spine for passive translation to the contralateral side when the spine is tested in flexion
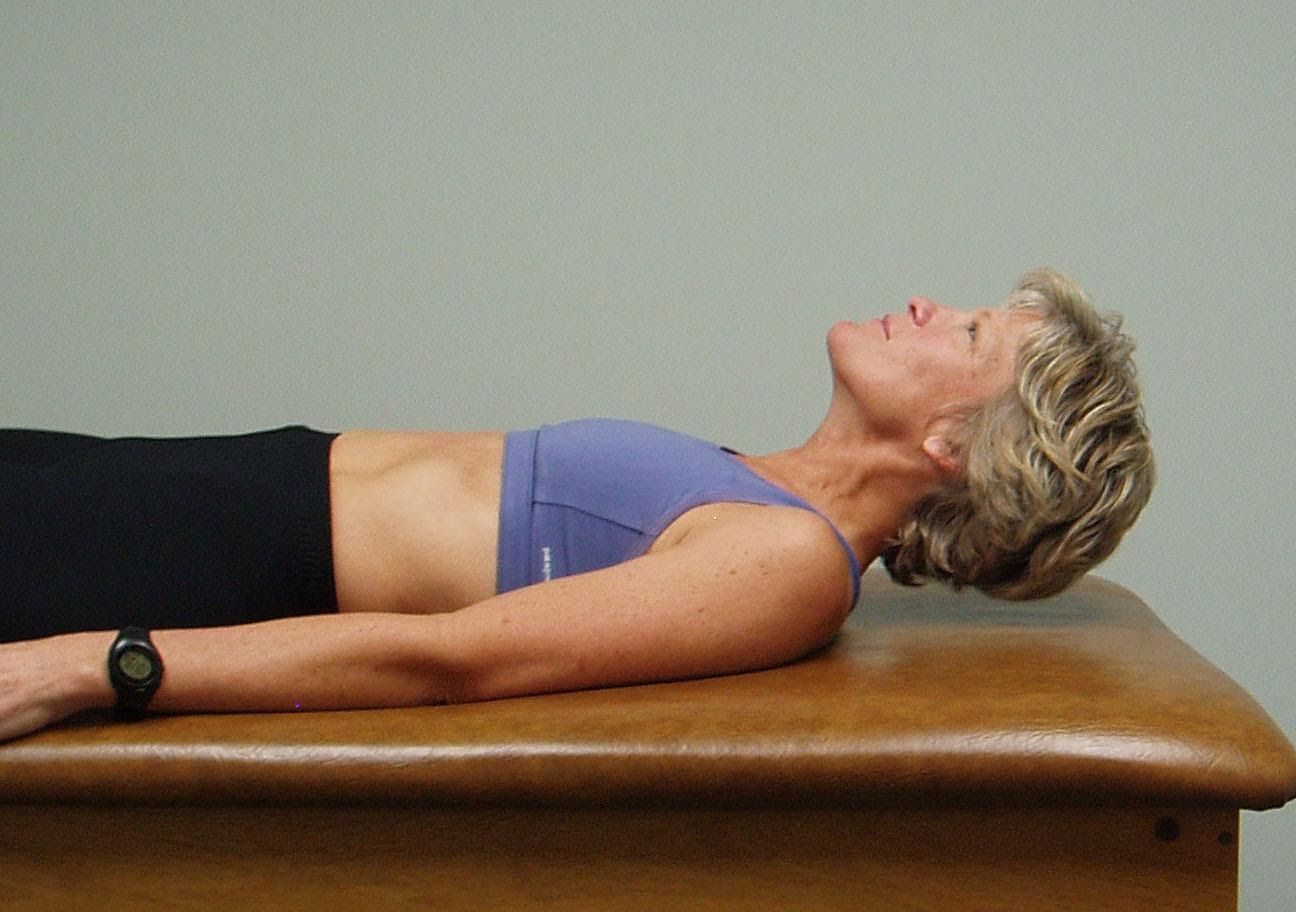
The patient is supine with legs straight and arms down to the sides.
Ask the patient to raise the head off the table and look down towards their feet.
Observe how the patient lifts the head, does the patient initiate the movement by progressive segmental flexion from above down or do they initiate the movement leading with the chin up?
Interpretation and the most common dysfunctional pattern seen
Normally the patient should be able to easily lift up their head and segmental flex thru the cervical spine utilizing their deep neck flexors throughout the full range of motion (pictured on the top)
The therapist watches for the chin to protrude forward indicating substitution by the sternocleidomastoid muscles for the inhibited deep neck flexors (pictured on the bottom).
If this movement is viewed as dysfunctional the therapist should then passively flex the neck to determine if this is a mobility problem or an inhibition problem. If passive ROM is restricted this is a mobility problem due to tight cervical extensors, an ERS dysfunction of the upper thoracic spine, hypertonic upper trapezius and/or levator scapulae, adverse neural tension, etc. If passive ROM of the cervical spine is free, but the active movement is dysfunctional think about a motor control/inhibition problem.
The patient is lying on their back and places one hand under the upper part of the neck, at the base of the skull.
Ask the patient to attempt to nod the chin down slightly, increasing the pressure against the hand under the upper neck. Instruct the patient to avoid pushing their head back toward the table.
There should not be any palpable tension in the superficial muscles in the front of the neck as they perform the exercise.
The patient is instructed to hold for 10 seconds and repeat 3-5 times, gradually working up to 10 repetitions.
In sitting, instruct the patient to palpate the muscles in the front of the neck.
Then instruct the patient in using the deep neck flexors by nodding their chin down slightly towards their chest. Explain to the patient to try to avoid activating the superficial muscles that their are feeling in the front of the neck.
Emphasize tucking the chin toward the chest rather than bending the head forward. Little actual movement of the head should occur if done correctly.
The patient may feel a slight stretch at the base of their head.
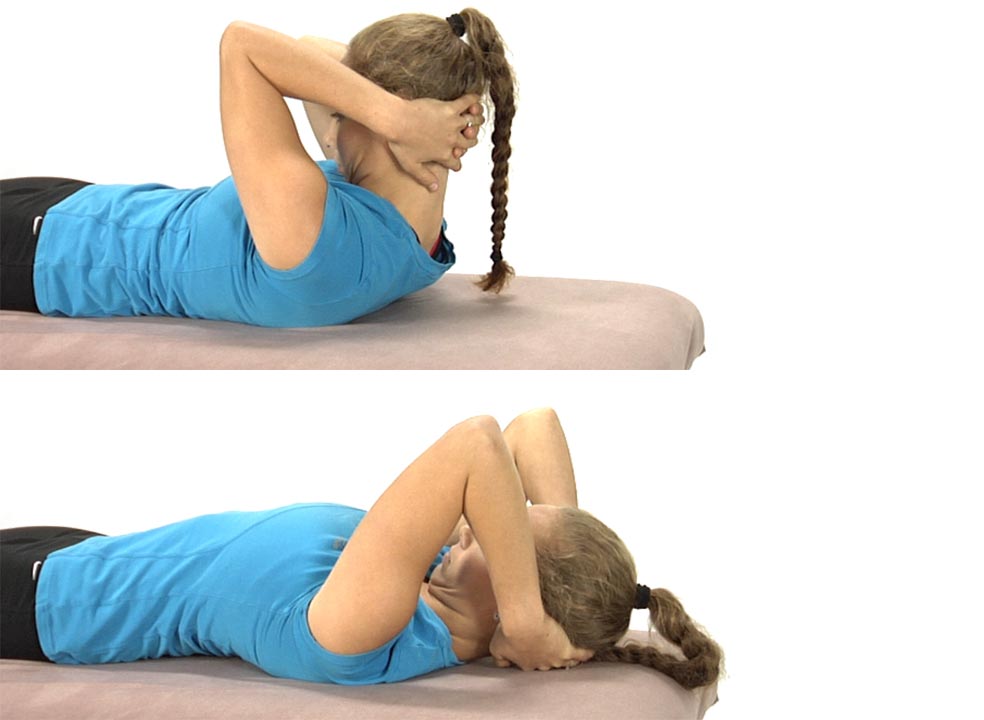
The patient is lying on their back with their hands clasped behind the head.
Instruct the patient to only use their arms to lift their head up so that the chin is drawn toward the chest and a stretch is felt through the back of the neck.
Once the head is brought up fully the patient is told to hold this position for 5-10 seconds, then slowly lower the head back to the table segmentally from below up, using the deep neck flexors eccentrically to lower the head back down to the table and assisting the movement with their hands as needed.
The hands only support the head as needed and an emphasis is placed upon keeping the chin down as the head is returned back to the table.
They repeat 3-5 times.
Eventually as the deep neck flexors become stronger, the hands should no longer be needed to assist in slowly returning the head back to the table.
The goal with this exercise is for the patient to be able to segmentally flex the neck and return back down to the table segmentally without using the hands to assist with the chin staying down throughout the entire movement.