Mobilization of the Thoracic Spine in the Lat Dorsi Stretch Position
In kneeling, have the patient place their elbows on top of a bench or chair and walk their knees back until their hips are flexed to approximately 90º.
Their hands and forearms should be together with the head resting on their upper arms.
Ask the patient to press the inner border of their arms together to separate the shoulder blades in back.
The patient is instructed to drop their chest toward the floor as much as possible, then perform a posterior tilt (12:00) of the pelvis without lifting up the chest. They should feel a good stretch along the sides, around their shoulder blades.
The therapist can then apply a posterior to anterior mobilization glide on the spinous process or transverse processes of any segment that appears to be restricted for extension while the patient maintains the stretch or the therapist can perform a myofascial stretch using the fists to draw the soft tissues towards the midline.
The goal is to increase extension in the mid to lower thoracic spine before instructing the patient in self-stretching of the latissimus dorsi.
Remember that the lower trapezius not only contributes to mobility of the shoulder, but is also a thoracic spinal extensor. Consequently studies have found that both mobilization and manipulation techniques to increase extension in the thoracic spine result in an increase in lower trapezius muscle strength, at least in the short term (Liebler et al., 2001 and Cleland et al., 2004).
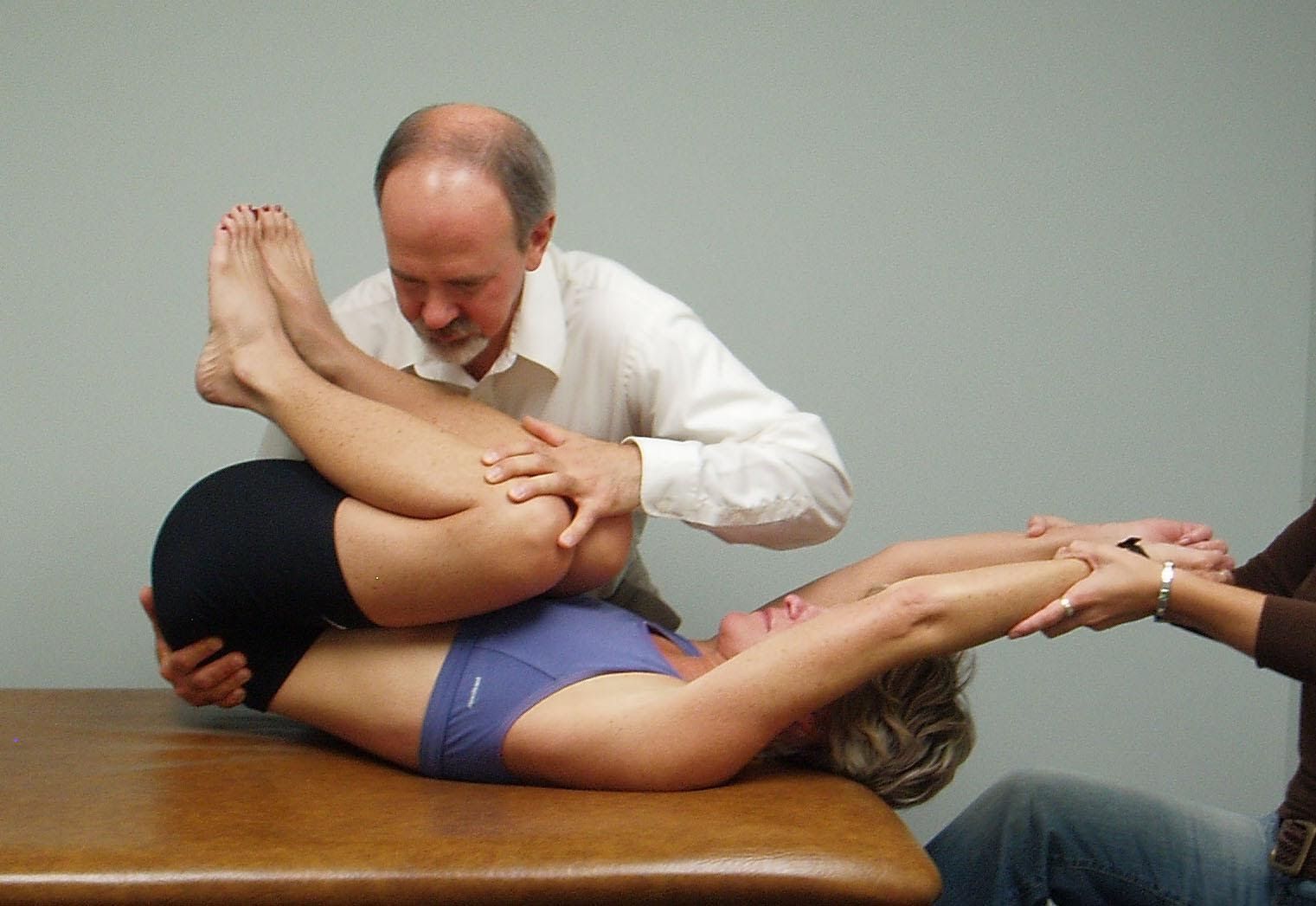
Dysfunctional Scapular Depression and Shoulder Flexion Tests
Anatomy and Biomechanical Considerations:
The scapular depression tests are used to evaluate the strength/tone of the lower trapezius muscle. The lower trapezius works together with the serratus anterior in a force couple that results in upward rotation, posterior tilt and external rotation of the scapula that is required during elevation of the arm. Note that the lower trapezius is also an extensor of the lower thoracic spine so with restricted thoracic spinal extension (FRS dysfunctions from T6-10) the lower trapezius is inhibited. When the lower trapezius is inhibited the patient may substitute by using the latissimus dorsi to depress the shoulder resulting in downward rotation of the scapula and limited external rotation of the humerus. In addition, hypertonicity in the latissimus dorsi contributes to increasing the thoracic kyphosis and the lumbar lordosis. The bilateral shoulder flexion test in supine allows us to evaluate the length of the latissimus dorsi as well as observe that when it’s hypertonic the patient will compensate by arching the lower back as the latissimus dorsi reaches its end range.
Therefore before attempting to retrain the lower trapezius we must assess for and treat any FRS Dysfunctions from T6-10 and lengthen the latissimus dorsi.
Lower Trapezius:
Attaches to the spinous processes and the interspinous ligaments from T4-T12 and along the medial border of the scapula and medial end of the spine of the scapula.
Function: It upwardly rotates, posteriorly tilts and externally rotates the scapula and assists in extending the thoracic spine from T4-T12.
Innervation: Spinal Accessory Nerve Cranial XI and the dorsal rami from T4-T12.
Inhibited by FRS Dysfunctions from T6-T12.
Latissimus Dorsi:
Attached to the lower 6 thoracic spinous processes and all the lumbar vertebrae, sacrum, crest of ilium and lower 3-4 ribs
Function: adduction and internal rotation of the shoulder, depression of the scapula; extension of lumbar spine and anterior tilt of the pelvis
The scapular stabilization tests are designed to assess the ability of the serratus anterior to hold the medial border of the scapula firmly against the thorax when loading is applied through the arms. If the therapist observes winging of the scapula with either one of these tests then the assumption is that the serratus anterior is weak/inhibited. Often when this occurs you’ll notice that the normal thoracic kyphosis is reduced with straightening of the upper thoracic spine. In extreme cases the upper thoracic spine appears lordotic. Multiple ERS dysfunctions from T3-5 are often found when this has occurred and they need to be addressed first before attempting to retrain and strengthen the serratus.
Anatomy and Biomechanical Considerations:
Serratus Anterior
Attaches from along the medial border of the scapula and especially to the inferior angle, to ribs 1-8 or 9
Functions: upwardly rotates, posteriorly tilts and externally rotates the scapula; protracts the shoulder or posteriorly translates the thorax resulting in flexion of the thoracic spine
Muscle Energy Technique for FRS Dysfunctions T6-10
For an FRS R from T6-10:
The patient places their R hand on their L shoulder and the therapist reaches under the patient’s R arm and grasps the patient’s L shoulder.
The therapist palpates the L side of the interspinous space monitoring the superior aspect of the inferior spinous process, ie., FRS R T8,9 the therapist monitors the superior aspect of the spinous process of T9 on the L side.
Initially the patient is sitting with their spine flexed and the therapist asks the patient to slowly sit up by pushing the belly forward to introduce extension from below up to the palpated interspinous space.
The therapist introduces slight L rotation down to the palpating finger.
The therapist then translates the patient from L to R to introduce L side bending without closing down and pinching at the interspinous space.
The patient attempts to R SB for 5-7 seconds which the therapist blocks.
When the patient relaxes the therapist repositions the patient to the new motion barrier by first standing up to decompress the segment, then rotating the patient to the L and finally translating the patient from L to R to the new L side bending barrier.
No pinching should be felt at the palpated segment by the therapist or the patient.
This entire sequence is repeated 3 to 4 times then mobility is reassessed.
Patients who present with complaints of neck and/or shoulder pain often state that one of their most pain provoking activities is raising their arm overhead. The shoulder abduction test helps us to determine if the patient has a normal or abnormal scapulo-humeral rhythm and to determine if their scapular stability is compromised when they raise their arm overhead. This test, if abnormal, may also indicate that the patient has abnormal neurobiomechanics with involvement of the brachial plexus. If this is the case the patient may hold their shoulder in an elevated position even when at rest and side bend their head to the ipsilateral side during the shoulder abduction test in an attempt to diminish tension on the plexus.
Anatomy and Biomechanical Considerations:
Normally during shoulder abduction the scapula upwardly rotates around an AP axis, posteriorly tilts around a horizontal axis running along the spine of the scapula and externally rotates around a vertical axis (Ludewig et al., 1996). This three-dimensional movement of the scapula occurs as a result of a force couple between the lower trapezius muscle working in tandem with the serratus anterior. If either of these muscles should become inhibited/weak then normal scapular mobility and stability is compromised.
According to Janda (1990) shoulder abduction also requires activation of the contralateral quadratus lumborum as part of the shoulder abduction muscle firing sequence. This would appear to be especially important at approximately 120 degrees of abduction, when the weight of the movement arm must be counterbalanced. Palpation of the quadratus lumborum during unilateral shoulder abduction is used to assess the appropriate firing of this muscle as part of the shoulder abduction test. In a dysfunctional test we often find that the ipsilateral rather than the contralateral QL will fire making it difficult for the patient to elongate that side of the trunk during abduction of the arm and result in compensatory superior translation of the scapula. Excessive superior translation of the scapula has been found in subjects with shoulder impingement (Lukasiewicz et al., 1999). Ipsilateral FRS dysfunctions at T12,L1 are most often the cause of hypertonicity in the quadratus lumborum and therefore must be looked for and treated, when present, before considering to stretch this muscle. A muscle energy technique to address the FRS dysfunction will often result in normalizing the tone of the ipsilateral quadratus and restore the ability of the contralateral quadratus to fire normally during shoulder abduction.
Considering the effect that dysfunction of the postural muscles, as described by Janda in the Upper Crossed Syndrome, can have upon scapular mechanics during shoulder abduction, we look for and most often treat the following:
Hypertonicity of the levator scapula and pectoralis minor that restricts posterior tilt of the scapula.
Hypertonicty of the levator scapula and upper trapezius that restricts upward rotation of the scapula.
Hypertonicity of the pectoralis minor that restricts external rotation of the scapula.
Hypertonicity of the ipsilateral quadratus lumborum that forces substitution by the upper trapezius and levator scapula resulting in excessive superior translation of the scapula.
Self-Stretching of the Upper Trapezius and Sternocleidomastoid
Upper Trapezius and SCM Stretch
These muscles extend the upper cervical spine, side bend toward the ipsilateral side and rotate the head to the opposite side
When tight these muscles may serve as long restrictors for mobility at C0-C1
To stretch the right upper trapezius and sternocleidomastoid:
Instruct the patient to position their head in flexion, side bending to the left and rotation to the right.
Their left hand is placed on top and around their head for support. Instruct the patient not to pull on the head with the left hand.
The right hand grasps the chair or bench behind the right hip.
The stretch is introduced by asking the patient to slowly lean forward and away and not by pulling on the head. They should feel a stretch over the top of the right shoulder and behind the ear.
Then instruct the patient to tuck the chin down (nod the chin) to add to the stretch which should be felt at the attachment behind the right ear.
Ask the patient to pull their right shoulder blade down and back to further increase the stretch.
They hold for 20 seconds and repeat 2-3 times. Have the patient alternate sides and stretch to symmetry as much as possible.
The patient is instructed to sit with the head positioned in flexion, left side bending and left rotation, as though looking down towards the left hip.
Their left hand is placed on top and around their head for support. Instruct the patient not to pull on their head with the left hand.
The right hand is placed behind the right hip and grasps the chair/bench.
Ask the patient to slowly lean forward and to the left to feel a stretch along the right side of their neck.
To facilitate a balance between the levator scapulae and ipsilateral lower trapezius, instruct the patient to pull their right shoulder down and back using the lower trapezius muscle. If done properly they should feel an additional stretch in the levator scapulae muscle.
They hold for 20 seconds and repeat 2-3 times on each side.
The patient is left side lying with the head positioned in flexion, left side bending and left rotation.
The operator’s right hand is placed on the lateral aspect of the neck from C1 through C4 to stabilize the cervical spine. The operator’s left hand is placed over the patient’s right shoulder in front of the clavicle so that the shoulder can be brought into posterior tilt with depression of the medial border of the scapula. The patient’s right hand should be placed upon and remain on top of the right hip.
The patient is instructed to raise the right shoulder towards their ear which is resisted by the therapist for five to seven seconds.
Upon relaxation further posterior tilt and depression of the scapula are introduced by the therapist.