Pectoralis Minor Length or Posterior Capsule Tightness
How to Perform
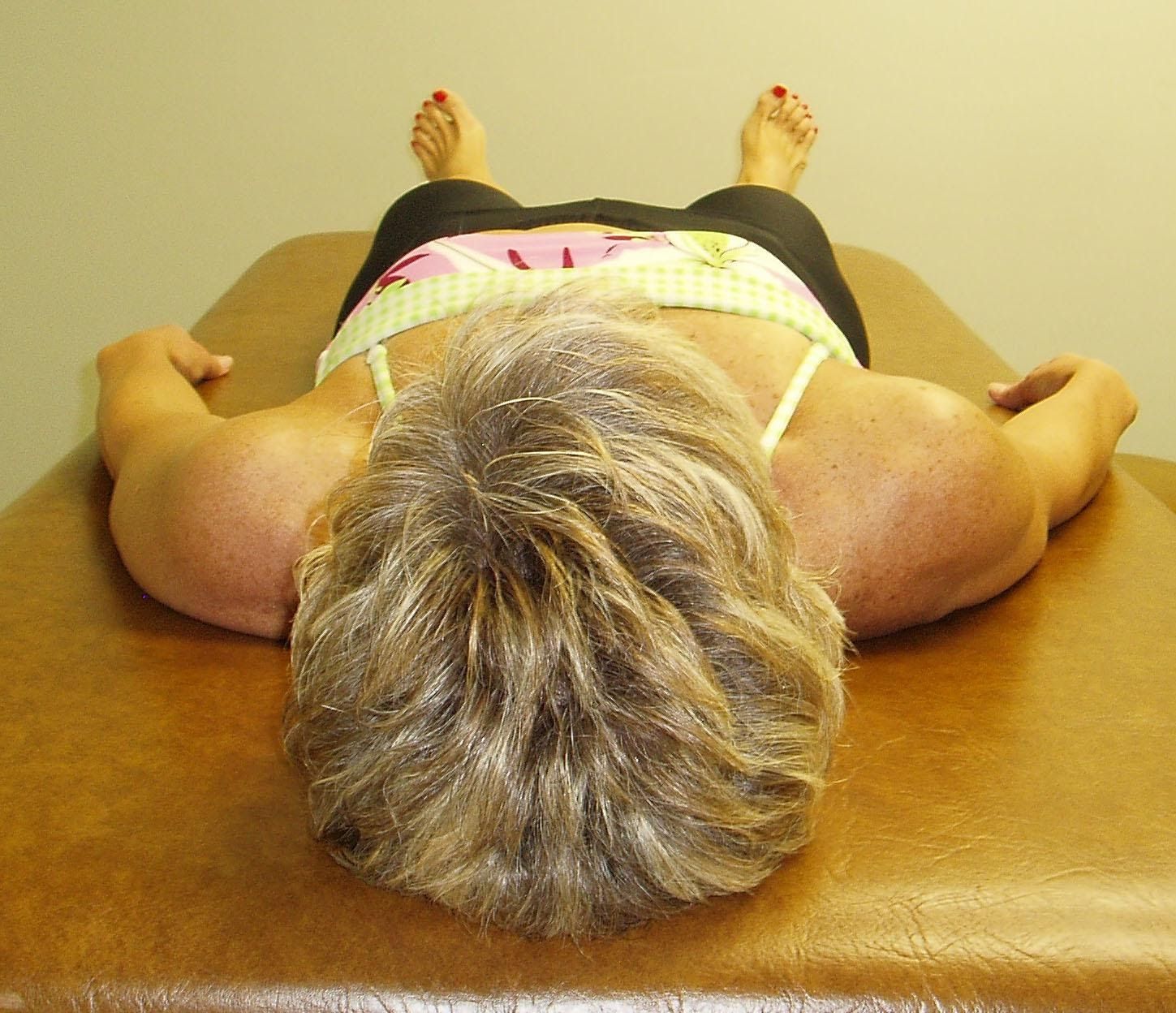
With the patient lying supine and without a pillow under the head, the therapist observes the relative position of both shoulders compared to the table top.
Notice that the right shoulder appears to be more anterior than the left.
Interpretation and the most common dysfunctional patterns seen
When observing that one shoulder appears to be relatively anterior compared to the opposite shoulder the therapist needs to determine the source of this anterior displacement. Is it due to a tight pectoralis minor as originally proposed by Kendall and McCreary, 1983 or due to a tight posterior shoulder capsule on that side, as the treatment for each of these dysfunctions is vastly different.
To differentiate between the two, the therapist applies an AP glide to the head of the humerus to confirm posterior capsule tightness on this patient’s right side. Recall that the pectoralis minor does not attach to the humerus so it should not influence or restrict posterior glide.
To assess for pectoralis minor hypertonicity as the cause of the anterior displacement the therapist can apply an inferiorly directed force on the anterior 3rd-5th ribs on both sides and note any resistance in extensibility between the two sides.
In this patient a restriction for AP glide of the right shoulder was noted indicating that the tissue involved is the R posterior capsule. Studies have shown that with a tight posterior capsule the head of the humerus is pushed forward and superiorly with a resultant loss of internal rotation mobility. (Harryman et al., 1990; Tyler et al., 1999; Tyler et al., 2000).
To confirm posterior capsule tightness the therapist then examines the range of motion for IR by placing the patient in side lying with the scapula stabilized. The arm is then passively internally rotated.