The patient assumes a hands and knees position with the hips centered over the knees and the shoulders centered over the hands.
Have the patient bend their elbows so that the shoulders are the same height as the hips and their head is held straight in line with the spine.
Instruct the patient to find a neutral lumbar spine position by rotating the pelvis anteriorly and posteriorly and positioning the spine in mid range. Then the patient draws the belly in without raising the back.
They hold the position for 5-10 seconds and repeat 3-5 times, increasing repetitions as their strength improves.
Watch the patient to make sure that the hips stay centered over the knees and the shoulders stay centered over their hands.
To increase the resistance, ask the patient to lift the L hand off the table slightly and hold for 5-10 seconds. Make sure that the patient keeps the right arm bent at the elbow as the tendency is to straighten the arm.
The patient is lying over a ball with their knees touching the floor. Instruct the patient to raise their arms up overhead with the thumbs pointing up towards the ceiling to make the letter Y. They hold for 5 seconds and repeat 5 times.
Then have the patient bring their arms up out to the side with the thumbs up to make the letter T. They hold for 5 seconds and repeat 5 times.
Next have the patient bring their elbows down towards their sides and raise the arms up to make the letter W. They hold for 5 seconds and repeat 5 times.
Finally, have the patient bring their elbows straight up towards the ceiling with the fingers pointing down towards the floor then ask them to externally rotate their arms and point the thumbs towards the ceiling to make the letter L. They hold for 5 seconds and repeat 5 times.
During each exercise the thumbs should be pointing up towards the ceiling with the arms parallel to their body during the holding period. Instruct the patient to gradually work up to one set of 10 repetitions of each exercise with the eventual goal being 2 sets of 10 repetitions of each exercise for a total of 80 repetitions.
The patient is kneeling with their hands placed on top of a bench or chair. Have the patient move their hips back until they are flexed to about 90º.
Instruct the patient to drop their chest down towards the floor so that their back is parallel to the floor (like a table top).
Their arms should be fully straight and their head in line with the trunk.
Ask the patient to lift their right hand off the bench with their thumb up (external rotation) and hold for 5-10 seconds.
They repeat 3-5 times initially, alternating arms. They gradually work up to 10 repetitions with each arm.
Watch to make sure that the patient does not raise up their back and/or drop their head when they lift the arm.
If with this exercise the patient reports feeling pain in the shoulder of their support arm, have them move their knees closer to the bench to unload the shoulder before they lift their other arm.
The patient is lying on their back with their hips and knees bent and feet resting flat on the floor. Their arms are at their sides with palms up.
Ask the patient to slowly bring the arms up along the floor keeping the shoulders and the backs of the hands always in contact with the floor.
They only raise the arms up as far as they can as long as they maintain contact with the floor.
If either hand or shoulder rises off the floor, the patient is told to stop and drop the arms back down a little. Then reach out with the arm on the restricted side to provide a longitudinal stretch before returning the arms back to the sides.
They repeat 3-5 times trying to bring the arms further up each time.
Goal: be able to sweep the arms along the floor with the shoulders and backs of the hands maintaining contact with the floor and the hands able to touch overhead.
Prone Lower Trapezius Strengthening – Bent Arm Overhead
To strengthen the right lower trapezius:
The patient is lying prone with their right arm bent and the palm of their right hand lying on the table above their head
Have them rest their forehead in the palm of their left hand
Instruct the patient to raise their right hand off the table as far as they can keeping their elbow and upper arm resting on the table/floor
They hold for 10 seconds and repeat initially 3-5 times increasing to 10 repetitions as they get stronger
The patient can be instructed to advance this exercise by raising the entire bent R arm off the table and hold for 10 seconds.
Tapping along the origin of the lower trapezius may help the patient “find” the muscle.
An alternative position is to have the shoulder abducted to 90 degrees with the elbow flexed to 90 degrees and the elbow resting on the table. From this position the patient externally rotates the shoulder lifting the hand off the table. This isolates the lower trapezius from the upper and middle trapezius better than any other exercise and avoids impingement of the shoulder that can occur in more elevated positions of the humerus (Ekstrom, Donatelli, Soderberg, 2003).
To retrain and strengthen the right lower trapezius:
The patient is lying prone with their left hand under their forehead and their right arm down at the side with the palm facing the ceiling.
Ask the patient to slowly lift their R shoulder up off the table/floor by bringing the shoulder blade down and back until their shoulder feels level with their back. The R hand remains on the table.
Make sure that the patient does not pinch their shoulder blades together, but that they draw the right shoulder blade down and back aiming towards their left back hip pocket.
They hold for 5-10 seconds and repeat 3-5 times initially. They add repetitions as their strength improves.
Make sure that the patient doesn’t depress the shoulder by using the latissimus dorsi.
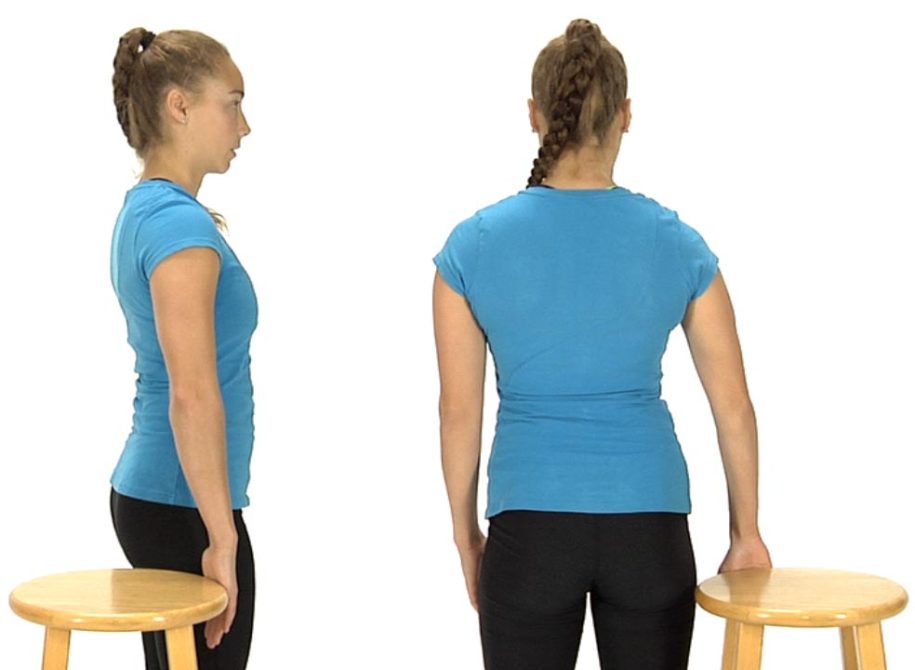
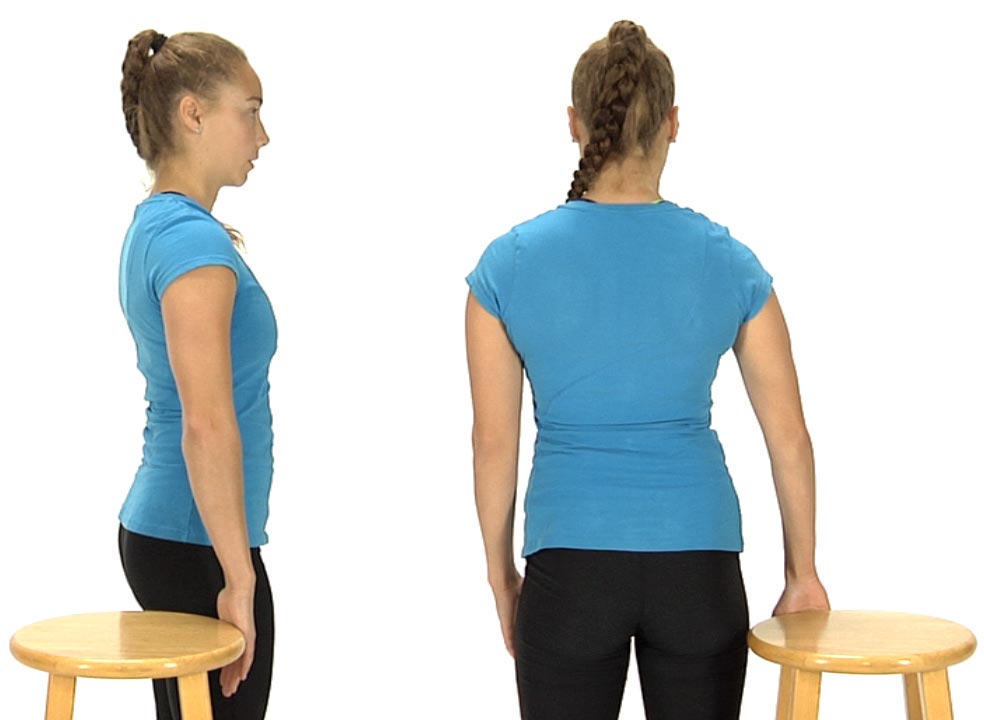
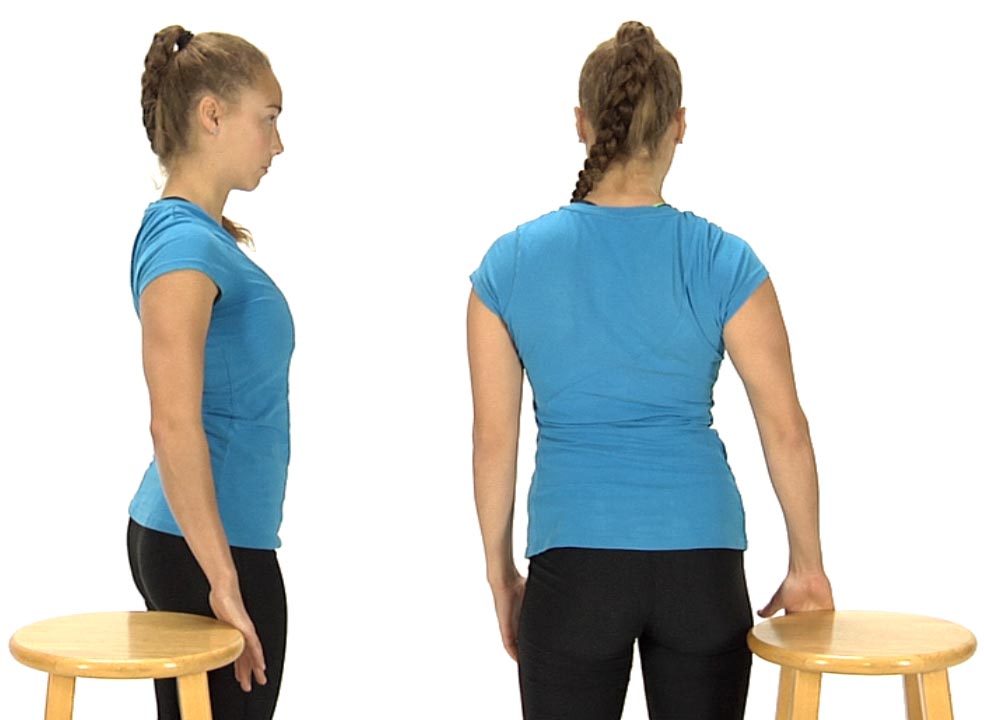
The patient is standing tall with an erect posture with the palm of their R hand facing behind them. Instruct the patient to gently push their R hand back into the edge of an immovable object such as a chair.
Ask the patient to inhale, then exhale as they push their R hand back into the chair, slightly extending through their mid-spine as they bring their R shoulder blade down and back. Do not let them overextend their lower or upper back.
Make sure that they keep their neck relaxed and they don’t hold their breath during the exercise.
Have them relax & slowly release and repeat 3-5 times initially, gradually increasing to 10 repetitions.
Dysfunctional Shoulder Abduction, Scapular Stabilization and Scapular Depression Tests
These three functional movement tests are interrelated and therefore are addressed together when retraining is required because to normalize shoulder abduction the patient must be able to recruit with sufficient strength the normal force couple provided by the coactivation of the lower trapezius and serratus anterior muscles.
Anatomy and Biomechanics:
Normally during shoulder abduction the scapula upwardly rotates, externally rotates and posteriorly tilts, occurring as a result of a force couple involving the lower trapezius and serratus anterior. When these muscle groups are inhibited there is a loss of scapular stability and dysfunctional scapular mobility during elevation of the arm. The strength of the inhibitory influence by non-neutral spinal dysfunctions on these two muscle groups has not been fully appreciated by most clinicians. This is particularly true when attempts are made to “strengthen” the lower trapezius in the presence of a lack of spinal extension mobility that occurs secondary to FRS (flexed, side bent and rotated) dysfunctions. FRS dysfunctions from T6 thru 10 inhibit the ipsilateral lower trapezius. Likewise, ERS (extended, side bent and rotated) dysfunctions from T3-5, which limit thoracic flexion mobility, inhibit the serratus anterior. The result of this spinal inhibition on the lower trapezius and/or serratus anterior is that compensation is made by the levator scapula and upper trapezius and results in elevation, downward rotation and anterior tilt of the scapula. Also, restricted T3-5 rib mobility for anterior to posterior glides contributes to hypertonicity of the ipsilateral pectoralis minor resulting in protraction, internal rotation and anterior tilt of the scapula. The net effect of these muscle imbalances on the scapula results in an anteriorly tilted, downwardly rotated and medially facing glenoid fossa with impingement of the rotator cuff occurring during shoulder abduction.
Lower Trapezius
Attaches to the spinous processes and interspinous ligaments fromT4-12 and the medial end of the spine of the scapula
Functions: Upwardly rotates, posteriorly tilts and externally rotates the scapula and can assist in extension of the thoracic spine
Innervation: Spinal Accessory nerve, Cranial XI and the dorsal rami from T4 -12
Inhibited by FRS dysfunctions from T6-10
Serratus Anterior
Attaches from along the medial border of the scapula and especially to the inferior angle, to ribs 1- 8 or 9
Functions: upwardly rotates, posteriorly tilts and externally rotates the scapula and can assist in flexion of the thoracic spine
Mobilization of Adverse Neural Tension on the R side of the Cervical Spine
The therapist introduces translation from right to left with his/her contact on the dysfunctional articular pillar.
The patient is instructed to slowly abduct their R arm along the table as far as they can while the therapist maintains the right to left translated position of the cervical spine and prevents the dysfunctional segment from translating back to the right.
This is repeated several times. Each time the patient lowers their arm to their side the therapist takes up any additional slack for right to left translation.
Goals for treatment: translation from right to left at the previously noted dysfunctional segment is now free and the patient should be able to fully and comfortably abduct the right shoulder overhead without the therapist feeling the cervical spine translate to the right at any segmental level.