To treat an ERS Right and/or high tone in the Right Erector Spinae:
The patient starts this exercise in the hands and knees position and is instructed to sit back diagonally as though attempting to sit onto their right hip.
Instruct the patient to sit back as far as they can without holding onto the table with their hands.
Have them hold the position for 5 seconds then come back up to the original hands and knees position without pulling up with their arms.
Muscle Energy Technique: ERS Dysfunction in the Lower Thoracic Spine
The therapist places their L index and middle fingers on the L side of the spinous processes and translates the spine towards him looking for any restriction in L to R translation (L side bending). If the restriction is worse in flexion and improves in extension the diagnosis is an ERS R.
To treat the ERS R the therapist has the patient sit up tall initially, then introduces flexion from above down and below up creating an apex for flexion at the palpated segment. L side bending is then introduced by translating the patient’s shoulders from L to R to the feather edge of the L side bending barrier. The patient is instructed to gently side bend to the R for 5-7 seconds and then relax.
The therapist takes up the slack by further translating the shoulders to the R. This is repeated 3-4 times.
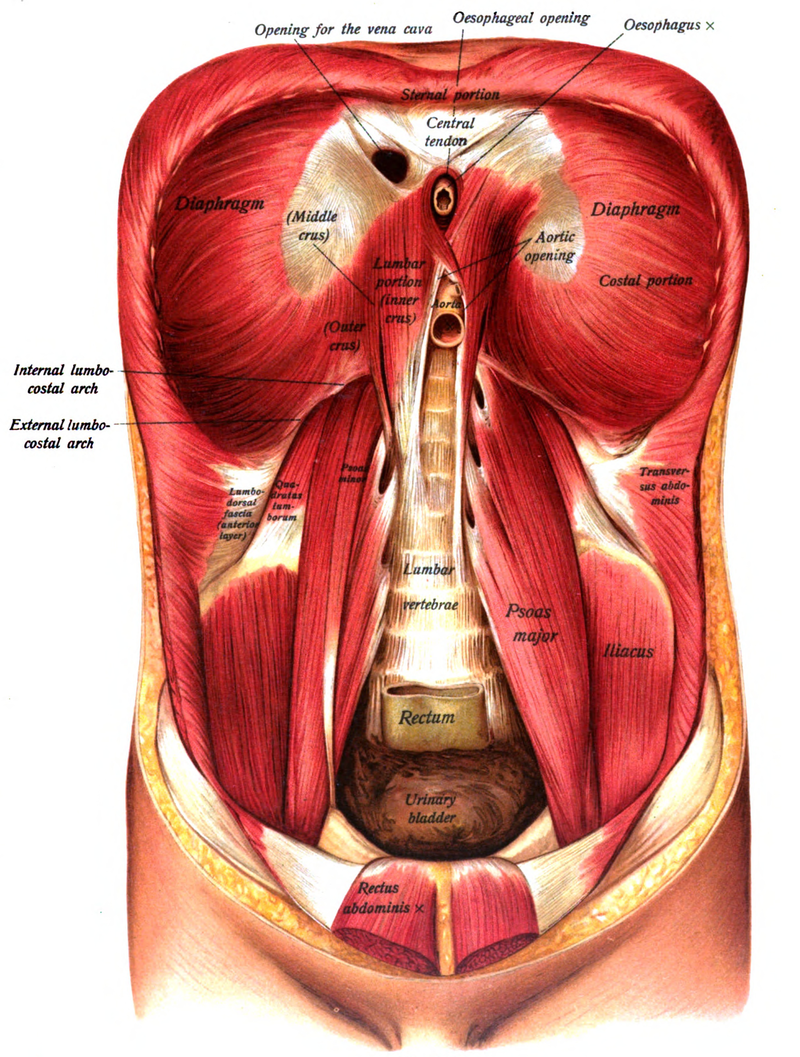
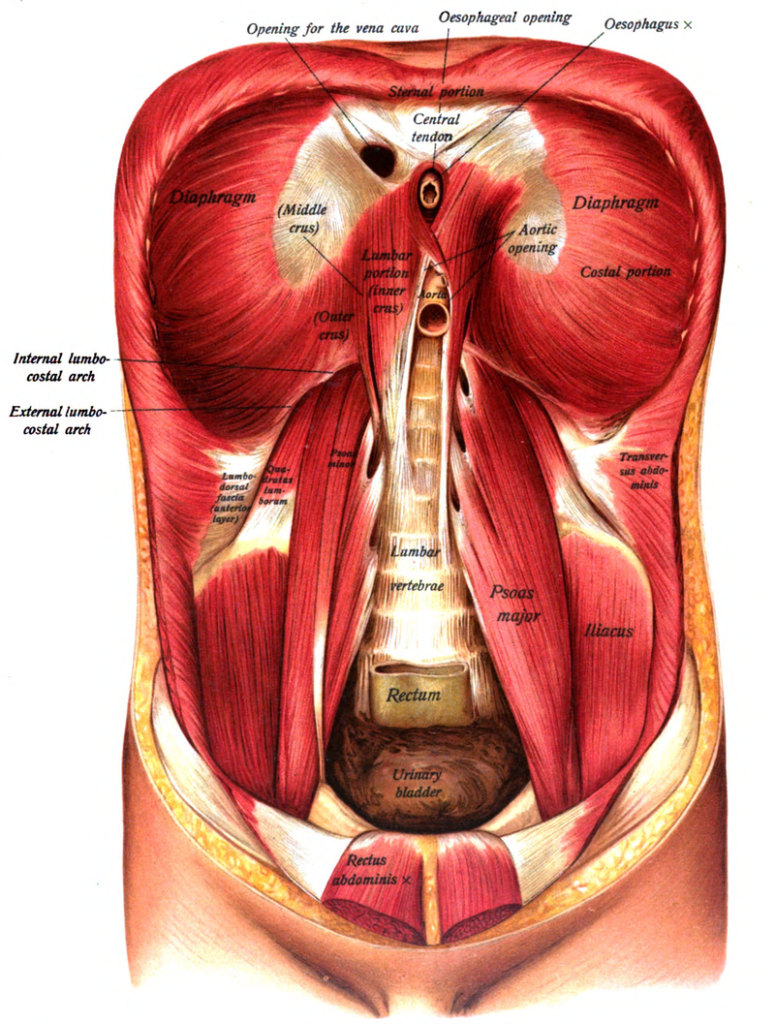
Psoas attaches to the transverse processes and vertebral bodies from T12 to L5 Iliacus attaches to the iliac fossa and sometimes anterior sacral base Powerful hip flexor and slight ER of the hip, side bends the LS to the same side and rotates away, when hypertonic these muscles limit hip extension Innervation: Femoral nerve – L2, 3 and 4
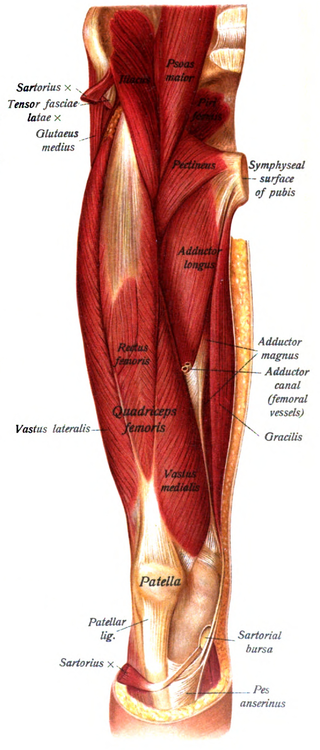
Tensor Fascia Latae:
Attached at the anterior iliac crest and ASIS Inserts into the IT band Flexes, abducts and internally rotates the hip, externally rotates the knee Innervation –Superior gluteal n. L4,5 and S1
Rectus Femoris:
Attached to the AIIS and the anterior hip capsule Flexes the hip and extends the knee Pain in the front of the knee cap is often a sign of a tight rectus femoris Innervation – femoral n. L2, 3, and 4
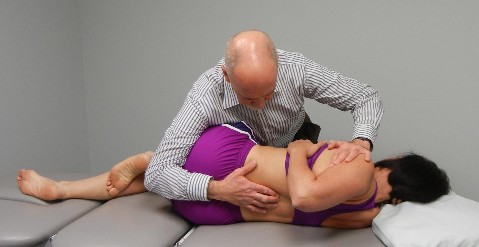
Patient is lying on their left side with their shoulders and hips square on the table and their hips flexed to 60 degrees with their lumbar spine in neutral.
You ask the patient to imagine a clock resting on top of their right hip so that 12 is closest to the shoulder and 6 closest to their feet, 3 is in front and 9 is towards the back.
You tell the patient that we are going to work from 1-2 o’clock (anterior elevation) down to 7-8 o’clock (posterior depression).
Start first by asking the patient to isometrically hold various positions along the diagonal from 1-2 down to 7-8 o’clock then work eccentrically giving you resistance as you pull down towards 7-8 or push up towards 1-2. You finish by asking the patient to pull the hip up towards 1-2 or push down and back towards 7-8 against your resistance.
The patient must avoid activating the right shoulder and right side of the neck during this activity and avoid moving out of the neutral position in their low back.
Manual Therapy for Restricted 9 o’clock – restricted pelvic rotation to the R and/or restricted sacral anterior nutation on the L
Treated as above except the patient is lying on their R side working through the pelvis from 10-11 o’clock (anterior elevation) down to 4-5 o’clock (posterior depression).