Dysfunctional Supine Heel Slide Test
Dysfunctional Supine Heel Slide Test
Anatomy and Biomechanics:
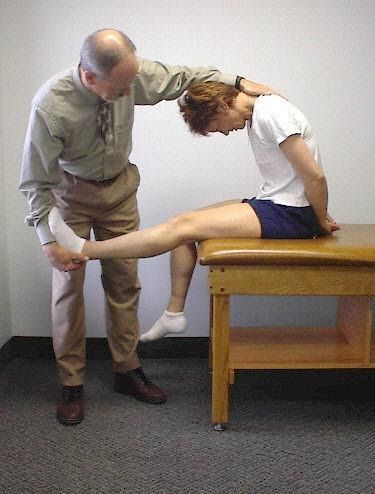
The ability to maintain a stable pelvis (level ASISs) while performing this functional movement test requires normal hip extension ROM and flexibility of the hip flexors with appropriate tone in the abdominal muscles. The abdominals must be strong enough to counterbalance the eccentric recruitment of the iliopsoas as the hip and leg are extended. An imbalance is seen when a hypertonic iliopsoas and weak abdominals results in an ASIS dropping inferiorly during the heel slide test.
After addressing any tightness in the anterior hip capsule, lengthening the hip flexors and mobilizing the femoral nerve as presented in module #3, then proceed to retraining the abdominals.
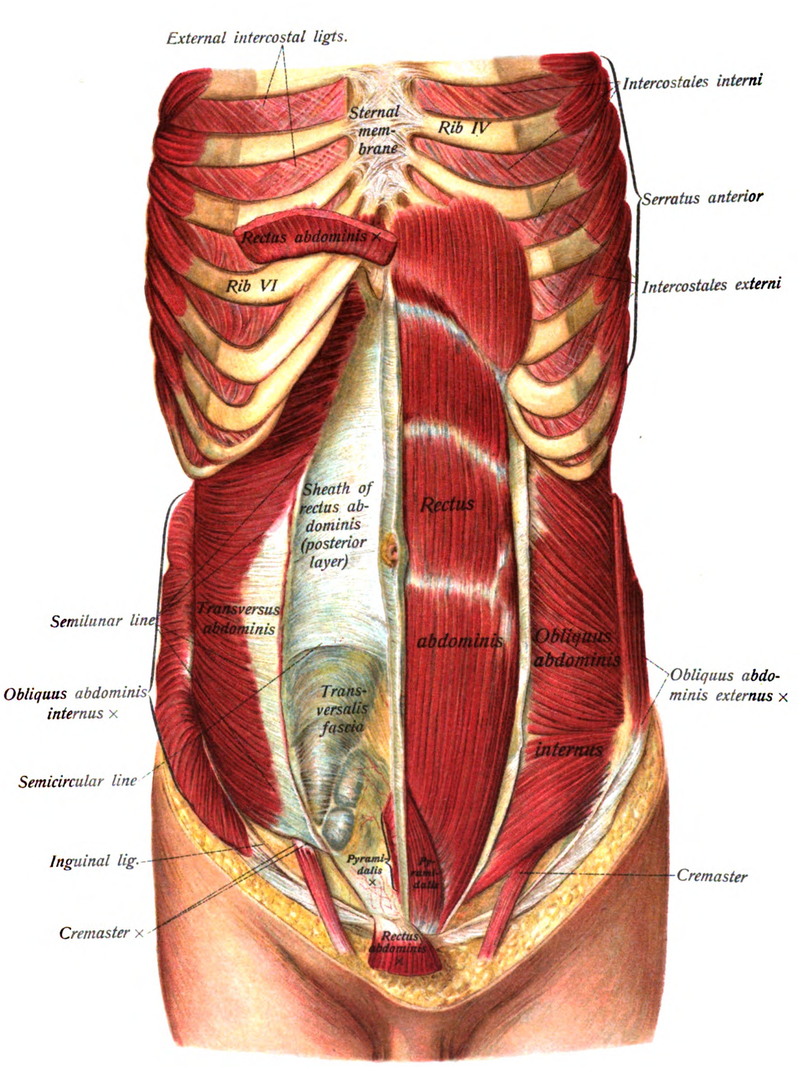
The Abdominals and Multifidi:
Global mobilizer in the sagittal plane – rectus abdominis
Global mobilizer in the transverse plane– internal and external obliques
Segmental stabilizer in the transverse plane – multifidi
Segmental stabilizer in all three planes – transversus abdominis
Rectus Abdominis:
Global mobilizer – brings the pelvis towards the trunk or the trunk towards the pelvis.
This muscle does not contribute to core stability.
Innervation – 7th thru 12th intercostal nerves
Transversus Abdominis:
- First trunk muscle to normally fire before you move your leg or arm in any direction, but in patients with a history of low back pain the transversus muscle fires late during movement of the lower limb (Hodges and Richardson, 1998) or upper limb (Hodges and Richardson, 1999).
- The transversus appears to fire as part of a feedforward movement synergy pattern, but contrary to initial studies activation of this muscle is dependent on the direction of movement and often is not bilaterally symmetrical, (Allison, Morris and Lay, 2008)
- Innervation – 7th thru 12th intercostal nerves, iliohypogastric and ilioinguinal nerves
Substitution Patterns to watch out for during retraining:
To retrain this movement dysfunction the patient is first instructed in how to monitor and maintain palpable symmetry at the ASISs when rolling the pelvis towards 12 o’clock. Most commonly the patient has difficulty drawing the R ASIS superiorly when rolling the pelvis towards 12 o’clock as shown in 2b.
The therapist should also observe/palpate the ASISs/PSISs when first instructing the patient in transversus abdominis retraining to insure that when performing the exercises the ASISs/PSISs remain stable and that one ASIS or PSIS does not drift inferiorly or superiorly during the active abdominal and pelvic floor engagement that occurs with these exercises.