The patient is lying on their back with knees bent and feet hip width apart.
Instruct the patient to find a neutral lumbar spine, midway between the end range of 12:00 and 6:00 then draw the belly in towards the spine.
Ask the patient to lift the toes up and push the heels away to tighten the quadriceps, then lift the hips up off the table while maintaining a neutral spine.
Instruct the patient to tighten the buttocks muscles as they bridge up.
Don’t let the patient lift up so high that they arch the lower back and lose the neutral position.
Have the patient hold for 10 seconds and repeat initially 3-5 times.
As the patient become stronger, they can attempt to straighten one knee while in the bridge position. They hold for 10 seconds and alternate with the opposite leg before lowering to the table. Make sure the pelvis doesn’t drop and the hamstrings do not cramp. Cramping of the hamstrings is an indication that the gluteus maximus is not engaged enough and that this exercise is too advanced for the patient.
Pushing away with the heels activates the quadriceps to inhibit the hamstrings from working to hard.
The patient is lying on their stomach on a table top, positioned with their knees bent and feet flat on the floor.
Instruct the patient to find a neutral lumbar spine by rocking the pelvis towards 12:00 then 6:00, finding the midpoint in between. The therapist monitors the PSISs to insure that they are level in the frontal plane.
The patient is instructed to hold this position by drawing the belly button in towards the spine.
Ask the patient to extend one leg at a time, maintaining flexion of the knee and keeping a neutral lumbar spine. Make sure that the patient does not abduct or externally rotate the leg during hip extension and that the PSISs remain level.
The patient should feel their buttocks tighten during the movement. The therapist should also be able to palpate tone in the gluteus maximus during this exercise.
Make sure that the movement occurs in the hip joint, avoiding extension of the spine.
It may be helpful to instruct the patient to try and elongate the leg by reaching away with their knee as the hip is extended.
Have the patient hold for 10 seconds and initially repeat only 3-5 times. Alternate legs.
Closed kinetic chain facilitation of the gluteal muscles:
With the patient’s arms at their sides instruct the patient to advance the right leg as far forward as possible keeping their right foot approximately an inch off the floor as they bend the left knee. The patient then reaches back as far as they can with the right foot staying an inch off the floor.
Then ask the patient to reach with their right foot out to the side and finally to draw a star taking the right foot behind and to the left and forward to the right and finally back to the right keeping the right foot an inch off the floor each time and bending their left knee as far as possible.
Repeat in each direction 4 to 5 times, then repeat standing on the right leg.
Make sure to watch for any valgus deviation of the stance knee during this retraining, which should be avoided.
From the hands and knees position the patient is instructed to sit back diagonally toward their right hip as far as they can without holding on with the hands.
Make sure the patient elongates/lengthens the right side of the spine as they sit back.
Instruct the patient to hold for 10 seconds and repeat 3-5 times or they can alternate from one side to the other.
The patient should report that they feel their gluteal/buttocks muscles contract with this movement.
To increase ROM and gluteal recruitment instruct the patient to do the hands and knees quadratus lumborum/lat dorsi self stretch before this exercise.
Side Lying Hip Abduction with Elongation at the Wall
To strengthen the Left Gluteus Medius:
The patient is lying on their right side with their shoulders and hips up against a wall and the right knee bent with the right foot flat against the wall.
Patient places their left hand flat on the floor in front of them for support.
Keeping the left knee straight and the heel of their left foot touching the wall instruct the patient to slowly lift the leg up the wall.
To further facilitate the gluteus medius, have the patient reach away with their left leg (elongate) and turn the left knee slightly up towards the ceiling while lifting the leg.
They hold for 10 seconds and repeat 3-5 times initially.
The patient is instructed to avoid hiking their left hip up when raising the leg and to keep their left heel against the wall throughout the exercise to avoid substitution of hip flexion and IR by an overactive TFL and hip hiking by the quadratus lumborum.
Side lying hip abduction with both legs extended and not lying up against a wall was reported to produce the highest % of MVIC for the gluteus medius out of 12 exercises that are commonly prescribed for gluteal strengthening (DiStefano et al. 2009).
The patient is lying on their R side with their shoulders, hips and feet touching against a wall. The shoulders and hips are perpendicular to the table or floor and the hips and knees are flexed to 45-60 degrees.
Instruct the patient to draw in the abdomen using the transversus abdominis without holding their breath.
Ask the patient to lift the left knee toward the ceiling, keeping the feet in contact.
The instruction to the patient is to attempt to lift the leg up to touch the wall and then hold for 10 seconds.
The patient repeats the movement 3-5 times initially, then increases the number of repetitions as their strength improves.
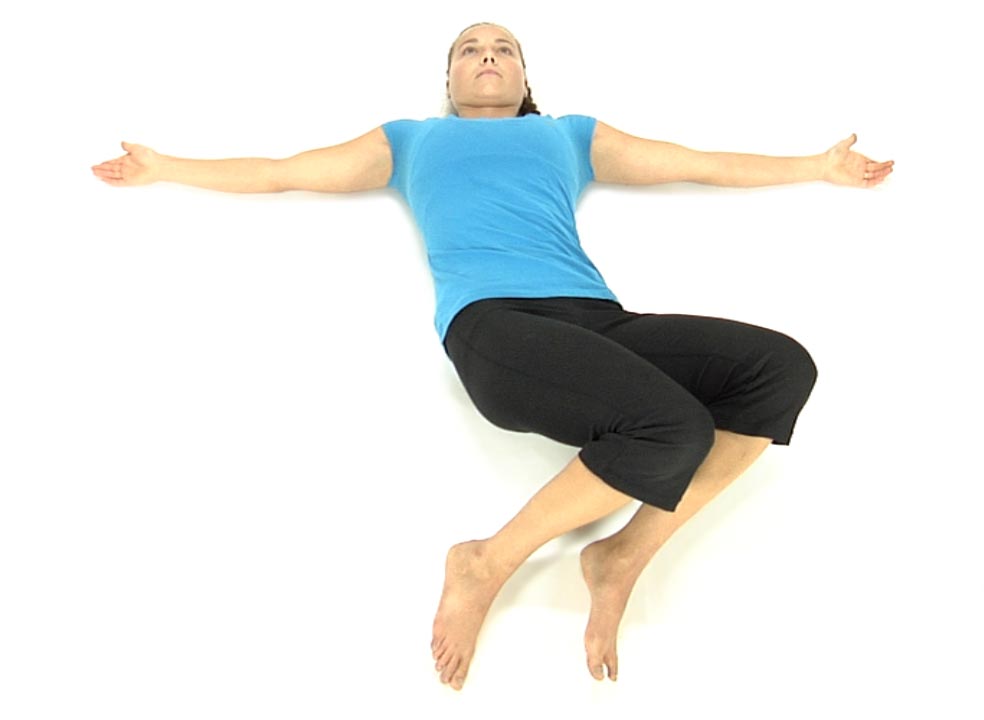
The patient is lying on their back with the knees and hips flexed and feet flat on the floor.
They are instructed to slowly drop their knees to the right approximately half way to the floor.
Ask the patient to slowly bring the knees back to the midline by flattening their back working from above down segmentally without engaging their hips, ie., T12, L1 then L2, etc. (Tell the patient to think about moving the pelvis towards 1 and 2 o’clock).
Once they’ve returned to the midline have the patient drop their knees slowly to the left, about half way to the floor.
Ask the patient to slowly bring the knees back to the midline by flattening their back working from above down segmentally without engaging their hips (Tell the patient to think about moving the pelvis towards 10 and 11 o’clock).
The patient repeats these movements alternating back and forth 3-5 times initially, gradually working up to 10 reps as their control/strength improves.
Make sure that the patient does not initiate the return to midline movement through the hips, but rather through the spine.