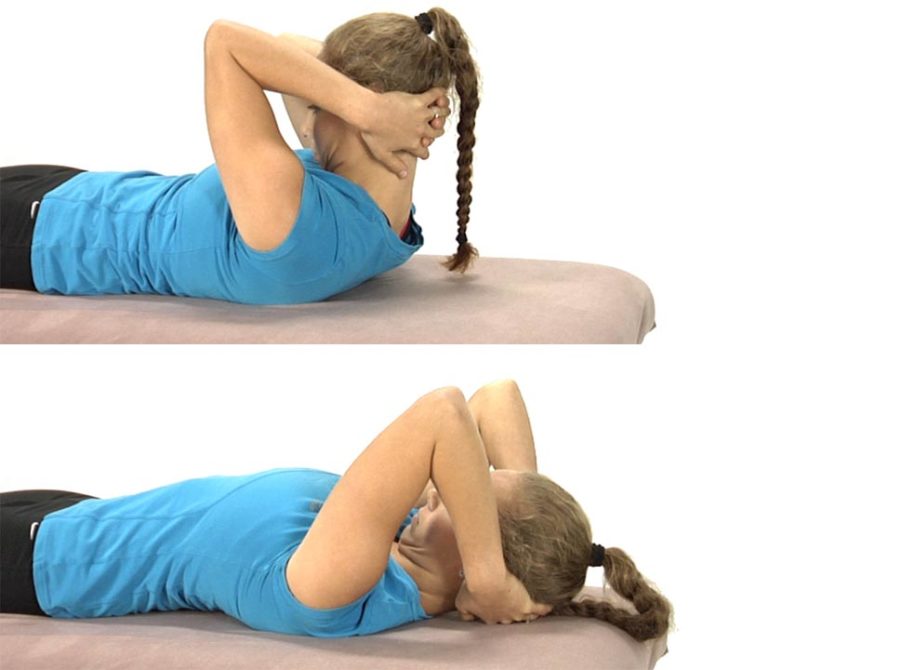
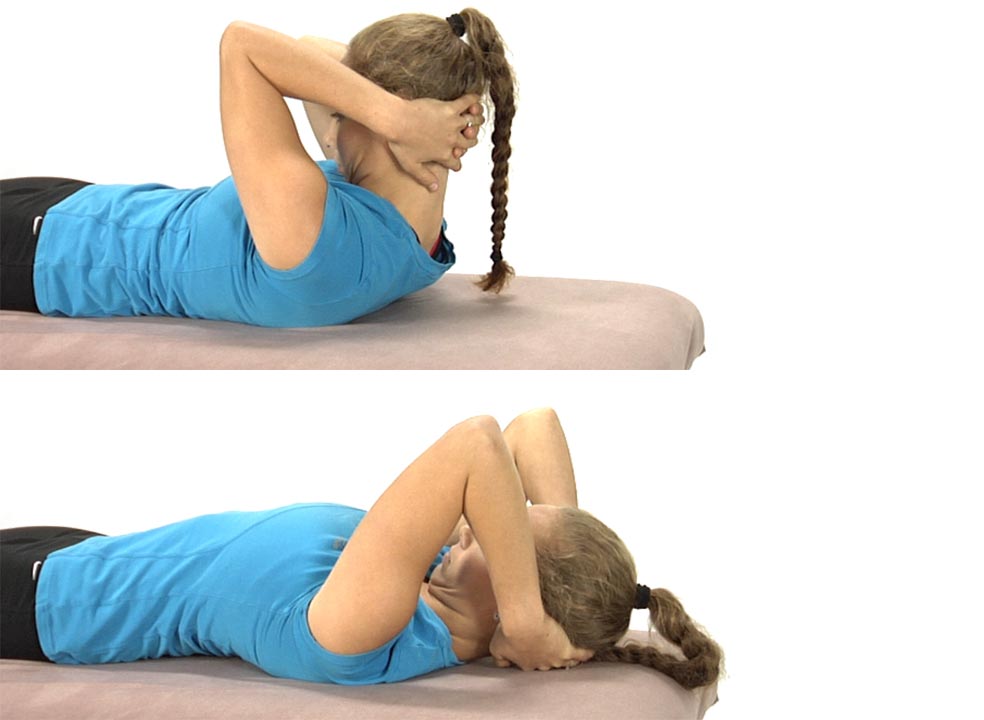
The patient is lying on their back with their hands clasped behind the head.
Instruct the patient to only use their arms to lift their head up so that the chin is drawn toward the chest and a stretch is felt through the back of the neck.
Once the head is brought up fully the patient is told to hold this position for 5-10 seconds, then slowly lower the head back to the table segmentally from below up, using the deep neck flexors eccentrically to lower the head back down to the table and assisting the movement with their hands as needed.
The hands only support the head as needed and an emphasis is placed upon keeping the chin down as the head is returned back to the table.
They repeat 3-5 times.
Eventually as the deep neck flexors become stronger, the hands should no longer be needed to assist in slowly returning the head back to the table.
The goal with this exercise is for the patient to be able to segmentally flex the neck and return back down to the table segmentally without using the hands to assist with the chin staying down throughout the entire movement.
Note: make sure that you can passively flex the patient’s cervical spine in supine lying through its full ROM without feeling any resistance before initiating retraining of the deep neck flexors.
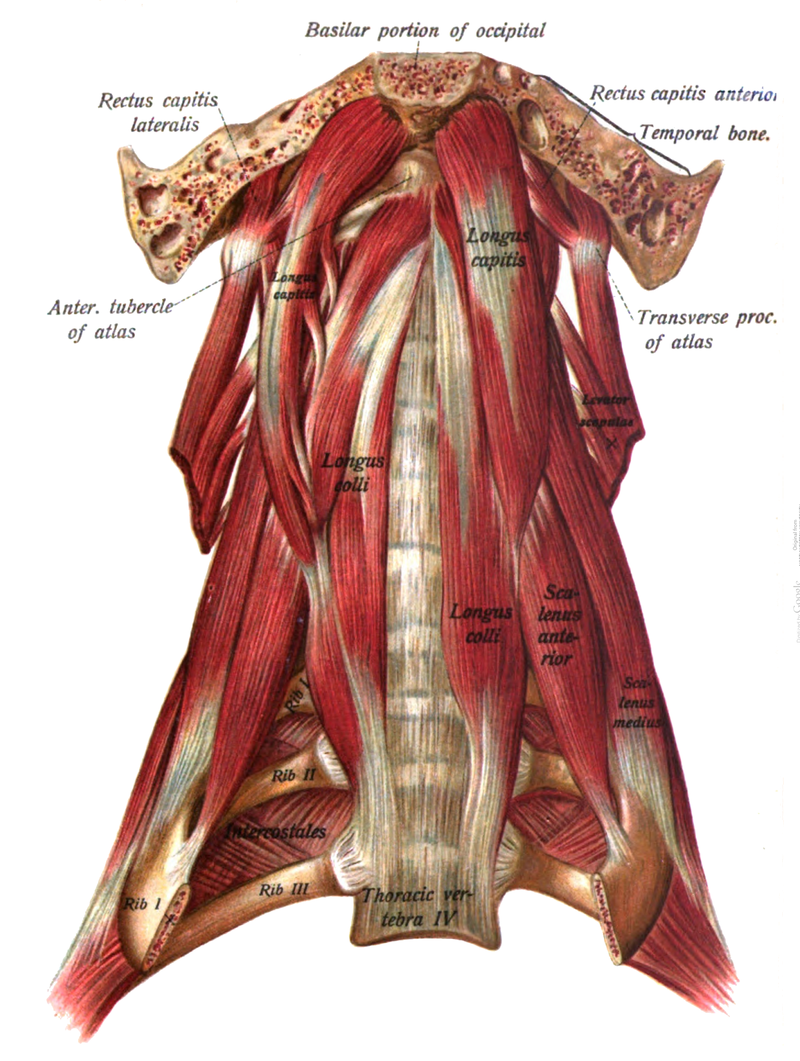
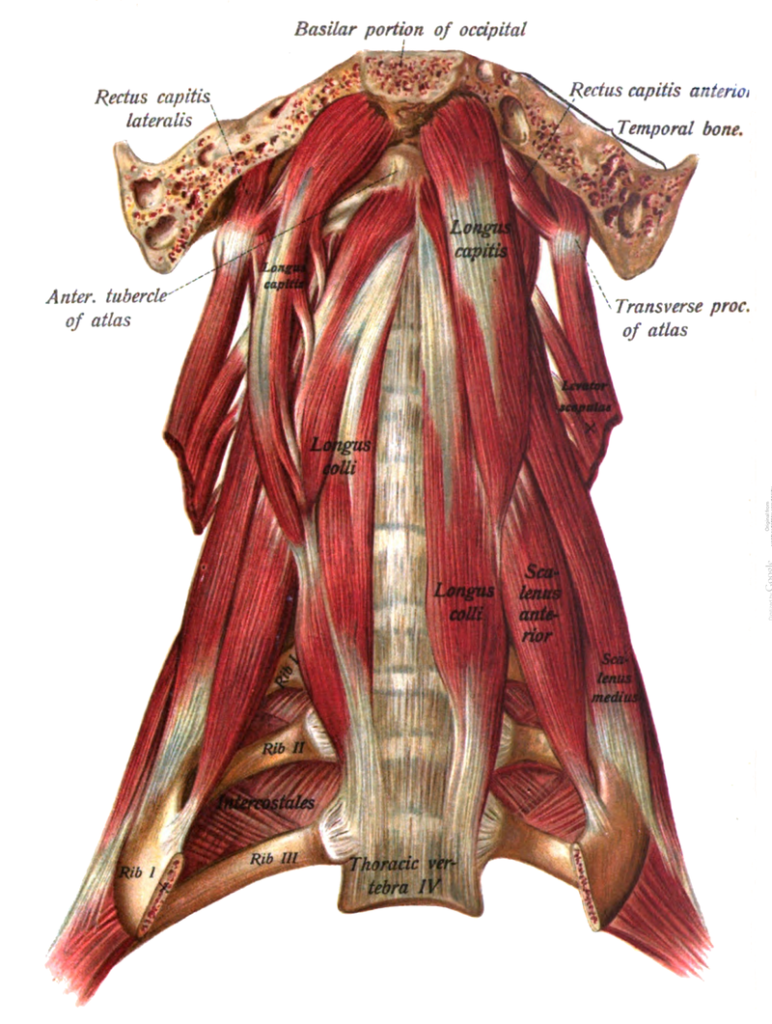
Retraining for this dysfunctional movement test focuses on improving the patient’s sensory awareness and ability to activate the deep neck flexors once the inhibiting factors for recruitment of these muscles has been removed. Therefore the exercises selected will depend upon the ability of the patient to “find” these muscles and recruit them appropriately.
Before attempting to retrain the deep neck flexors the sources of abnormal afferent input need to be addressed first. To review these sources and the recommended treatments see Module 6.
These muscles extend the upper cervical spine, side bend toward the ipsilateral side and rotate the head to the opposite side
When tight these muscles may serve as long restrictors for mobility at C0-C1
To stretch the right upper trapezius and sternocleidomastoid:
Instruct the patient to position their head in flexion, side bending to the left and rotation to the right.
Their left hand is placed on top and around their head for support. Instruct the patient not to pull on the head with the left hand.
The right hand grasps the chair or bench behind the right hip.
The stretch is introduced by asking the patient to slowly lean forward and away and not by pulling on the head. They should feel a stretch over the top of the right shoulder and behind the ear.
Then instruct the patient to tuck the chin down (nod the chin) to add to the stretch which should be felt at the attachment behind the right ear.
Ask the patient to pull their right shoulder blade down and back to further increase the stretch.
They hold for 20 seconds and repeat 2-3 times. Have the patient alternate sides and stretch to symmetry as much as possible.
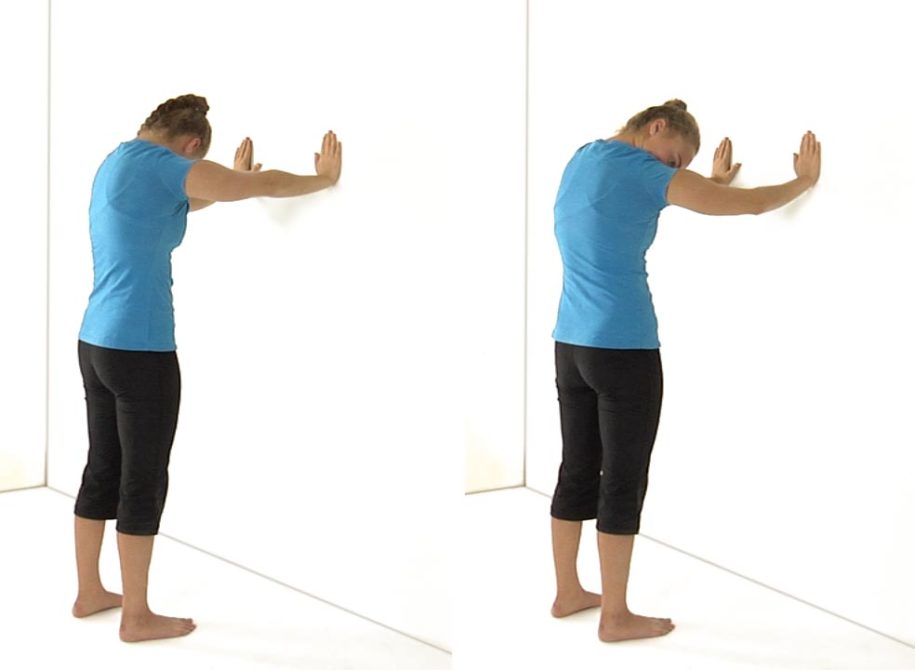
To Self-Mobilize ERS Dysfunctions in the Upper TS:
The patient is standing approximately three feet from a wall and places their hands on the wall at shoulder height.
Instruct the patient to drop their head down and push their arms against the wall fully extending their elbows and rounding their upper back. They should feel a stretch in their upper back.
Make sure that the apex of spinal flexion occurs in the upper and not the middle or lower back when they extend their arms.
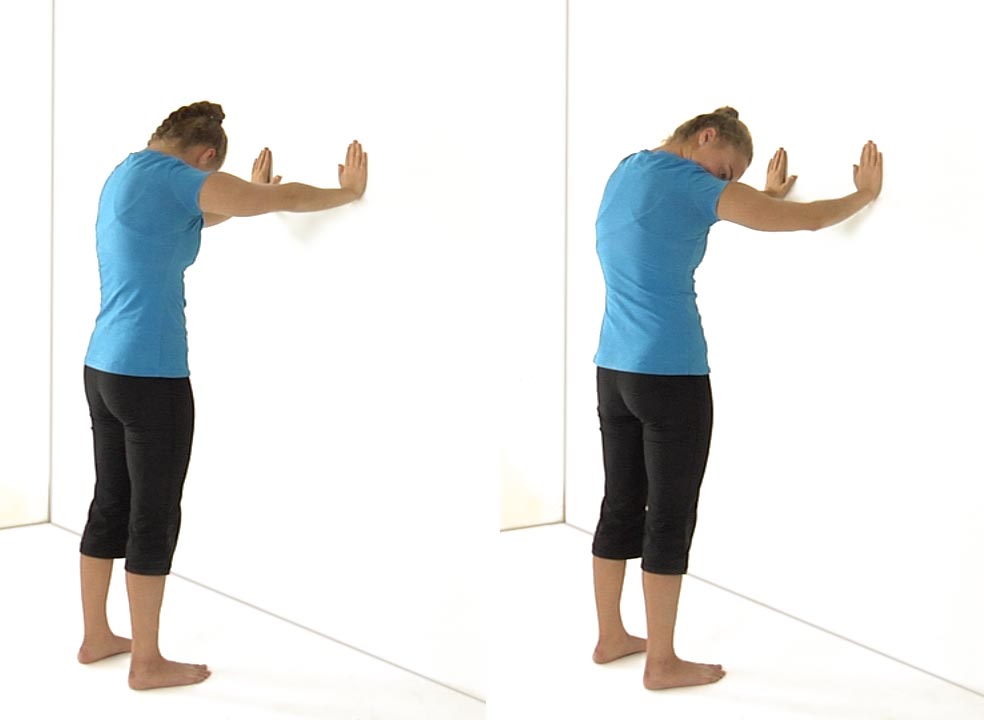
Instruct the patient to rotate their head to the R to stretch L sided ERS dysfunctions or rotate their head to the L to stretch R sided ERS dysfunctions as they extend their arms fully.
Ask the patient to hold for 5-10 seconds.
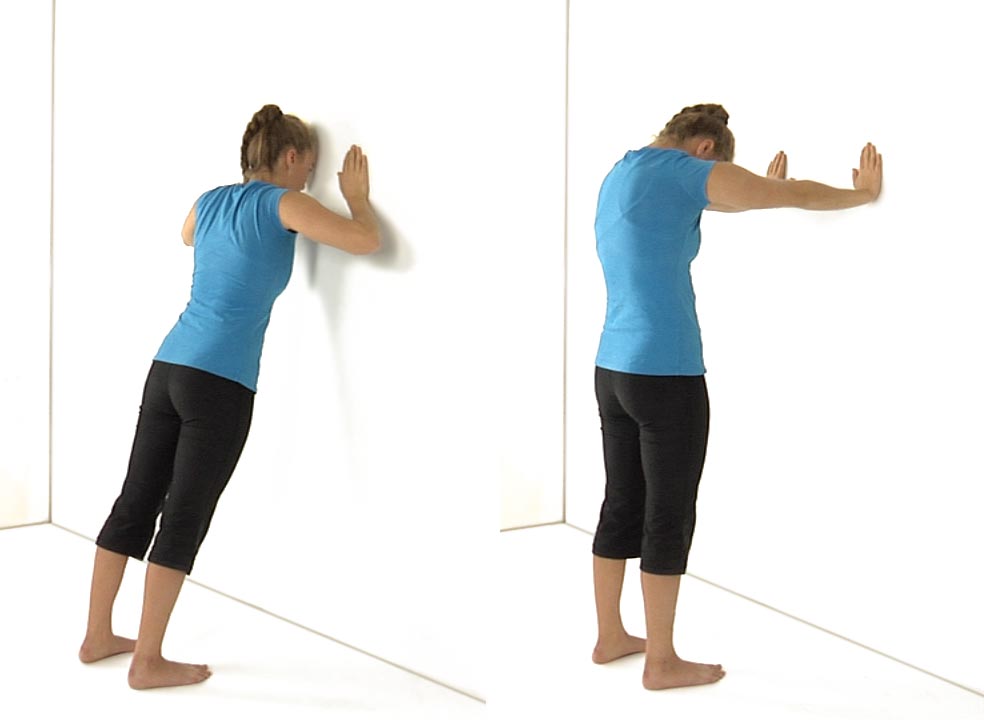
Then have the patient stand up straight and lean into the wall maintaining a neutral low back. Ask the patient to try to touch the wall with their forehead.
The shoulder blades should draw close together as they drop into the wall.
Instruct the patient to hold this position for 5-10 seconds and repeat the entire exercise 3-5 times.