From the hands and knees position the patient is instructed to sit back diagonally toward their right hip as far as they can without holding on with the hands.
Make sure the patient elongates/lengthens the right side of the spine as they sit back.
Instruct the patient to hold for 10 seconds and repeat 3-5 times or they can alternate from one side to the other.
The patient should report that they feel their gluteal/buttocks muscles contract with this movement.
To increase ROM and gluteal recruitment instruct the patient to do the hands and knees quadratus lumborum/lat dorsi self stretch before this exercise.
Side Lying Hip Abduction with Elongation at the Wall
To strengthen the Left Gluteus Medius:
The patient is lying on their right side with their shoulders and hips up against a wall and the right knee bent with the right foot flat against the wall.
Patient places their left hand flat on the floor in front of them for support.
Keeping the left knee straight and the heel of their left foot touching the wall instruct the patient to slowly lift the leg up the wall.
To further facilitate the gluteus medius, have the patient reach away with their left leg (elongate) and turn the left knee slightly up towards the ceiling while lifting the leg.
They hold for 10 seconds and repeat 3-5 times initially.
The patient is instructed to avoid hiking their left hip up when raising the leg and to keep their left heel against the wall throughout the exercise to avoid substitution of hip flexion and IR by an overactive TFL and hip hiking by the quadratus lumborum.
Side lying hip abduction with both legs extended and not lying up against a wall was reported to produce the highest % of MVIC for the gluteus medius out of 12 exercises that are commonly prescribed for gluteal strengthening (DiStefano et al. 2009).
The patient is lying on their R side with their shoulders, hips and feet touching against a wall. The shoulders and hips are perpendicular to the table or floor and the hips and knees are flexed to 45-60 degrees.
Instruct the patient to draw in the abdomen using the transversus abdominis without holding their breath.
Ask the patient to lift the left knee toward the ceiling, keeping the feet in contact.
The instruction to the patient is to attempt to lift the leg up to touch the wall and then hold for 10 seconds.
The patient repeats the movement 3-5 times initially, then increases the number of repetitions as their strength improves.
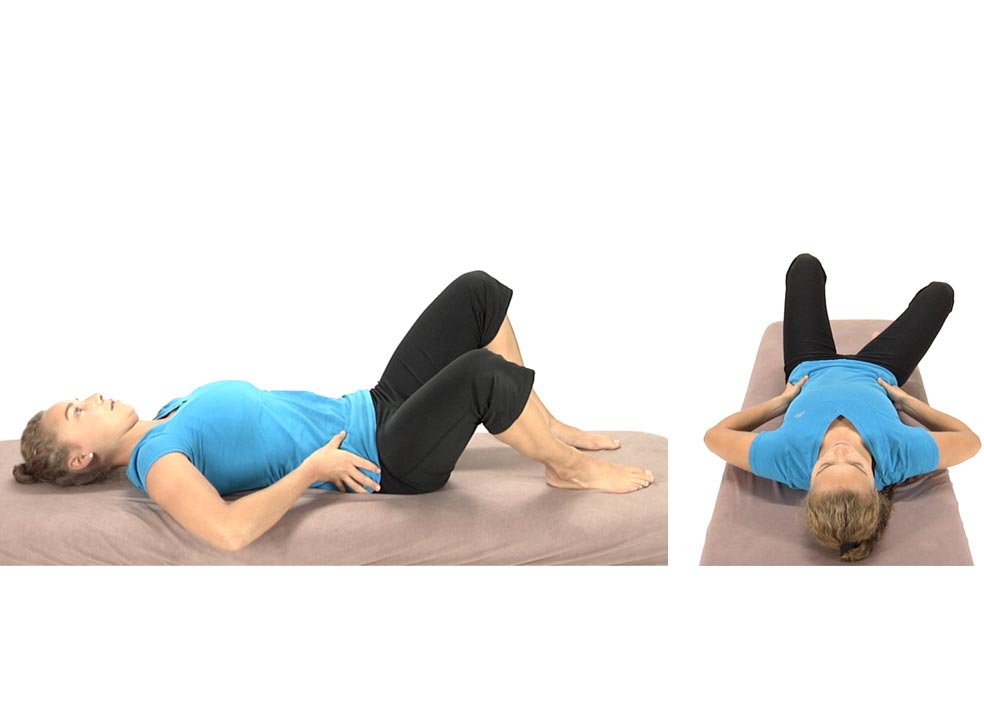
The patient is lying on their back with the knees and hips flexed and feet flat on the floor.
They are instructed to slowly drop their knees to the right approximately half way to the floor.
Ask the patient to slowly bring the knees back to the midline by flattening their back working from above down segmentally without engaging their hips, ie., T12, L1 then L2, etc. (Tell the patient to think about moving the pelvis towards 1 and 2 o’clock).
Once they’ve returned to the midline have the patient drop their knees slowly to the left, about half way to the floor.
Ask the patient to slowly bring the knees back to the midline by flattening their back working from above down segmentally without engaging their hips (Tell the patient to think about moving the pelvis towards 10 and 11 o’clock).
The patient repeats these movements alternating back and forth 3-5 times initially, gradually working up to 10 reps as their control/strength improves.
Make sure that the patient does not initiate the return to midline movement through the hips, but rather through the spine.
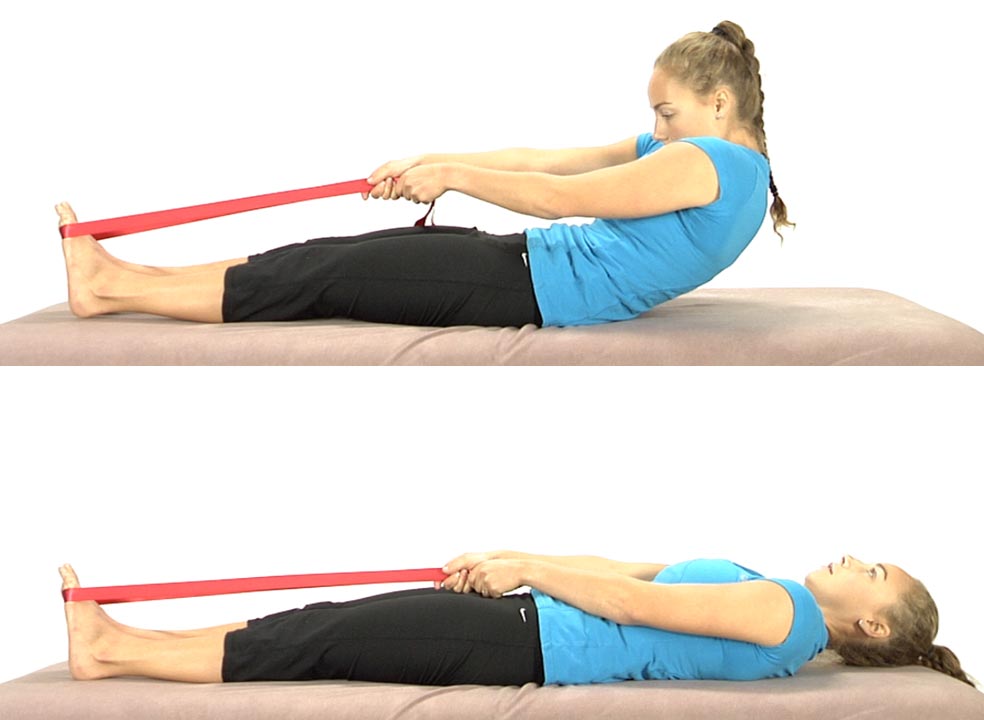
The patient starts in the long sitting position with a belt wrapped around the balls of the feet.
Instruct the patient to slowly slump back as though trying to touch their spine to the table segmentally from below up (S1, then L5, L4 etc.).
Emphasis is placed on posterior translation at each segmental level.
They’re only allowed to roll back as far as they can while maintaining spinal flexion.
Once they are able to control segmental flexion eccentrically then they can roll all the way back to the table and then come back up using the belt to assist as needed.
Have the patient repeat the exercise 8 to 10 times trying to work a little further back each time.
Goal – Eventually the patient should be able to roll all the way back and curl back up with segmental flexion without needing to use a belt to assist and without extending the spine while curling up.
Belt Assisted Eccentric Curl Backs with Therapist Assist
The patient starts sitting upright with a belt wrapped around the balls of the feet.
The patient is instructed to slowly slump back as though they are trying to touch their spine to the table segmentally from below up (S1, then L5, L4 etc.).
The therapist uses manual contacts to the abdominals and also to the spine to bring sensory awareness to specific levels of the spine as the patient proceeds.
Emphasis is placed on posterior translation at each segmental level.
The patient is only allowed to roll back as far as they can while maintaining spinal flexion.
Once they can control segmental flexion eccentrically then they can roll all the way back to the table and then come back up using the belt to assist as needed.
The patient is lying on the back, with their thumbs placed above the ASISs to monitor pelvic stability.
The patient is instructed to find the midpoint between 12:00 and 6:00 o’clock then draw the belly in towards the spine without flattening the low back so that they maintain a neutral lumbar spine.
The patient continues to monitor the position of the ASISs as they slowly drop the right knee out to the side.
The patient is instructed that if the R ASIS drops inferiorly when compared to the L ASIS while abducting and externally rotating the R hip they are to return back to the midline and start over.
The patient is instructed not to drop the R knee out to the side further than they can maintain leveling at the ASISs.
Repeat on both sides for 3-5 repetitions to start, increasing to 10 reps.
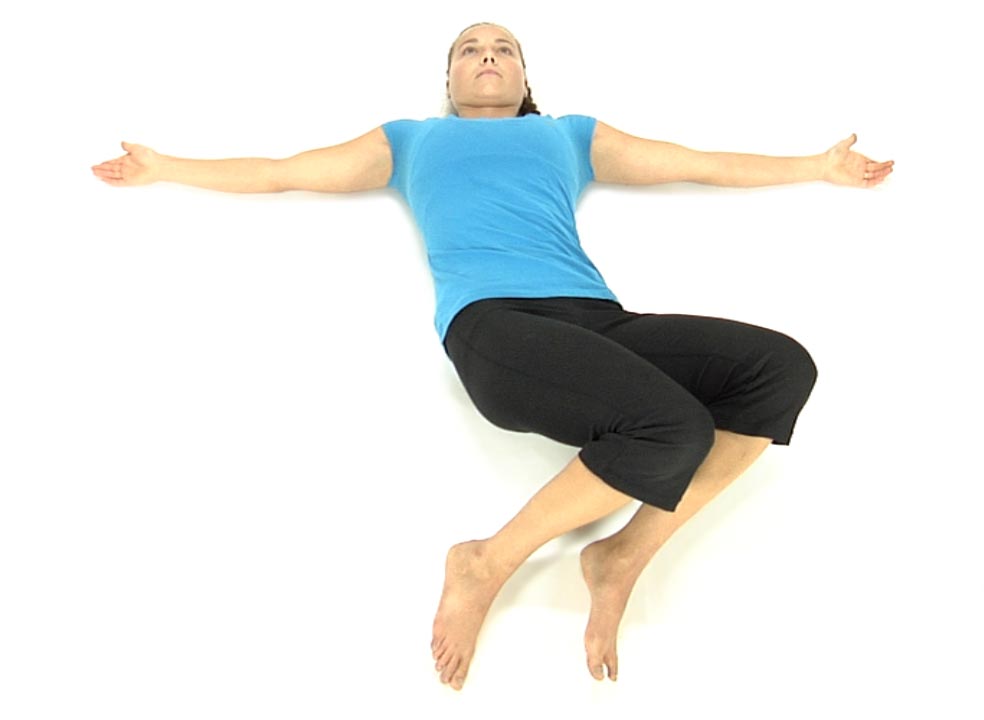
Bilateral Hip Abduction and External Rotation with a Neutral Lumbar Spine
The patient is lying on their back and instructed to find neutral, midway between 12:00 and 6:00 while monitoring the ASISs with their thumbs.
Instruct the patient to maintain neutral and draw the belly in towards the spine without flattening the low back.
While monitoring the ASISs with their thumbs ask the patient to slowly separate the knees while keeping the ASISs still/level.
If either ASIS begins to move inferiorly (towards the feet) instruct the patient to stop and bring the knees back to the midline and start over.
Repeat 3-5 times
The goal is for the patient to be able to maintain a neutral lumbar spine and symmetrically abduct and externally rotate both hips without either ASIS moving inferiorly.
The patient is lying on their back with both hips flexed to approximately 90º. Ask the patient to find a neutral lumbar spine by having them roll the pelvis from 12 to 6 and find the midpoint.
The patient monitors the ASISs with their thumbs to keep them level.
Instruct the patient to slowly touch one heel to the table, alternating between the right and left sides while monitoring the ASISs and not allowing an ASIS to drop inferiorly on either side.
As their strength improves, they can start extending the hip out further to touch the heel (bottom picture).
Have them repeat 3-5 times and increase repetitions as their strength improves.