Patient attempts to rise straight up off the floor just a couple of inches and holds for 30 seconds, alternating legs and repeating 3-5 times on each side.
Instruct the patient to come straight up and maintain a 90 degree angle at both knees as much as possible.
They can increase the level of difficulty by placing a wobble disc under the R foot.
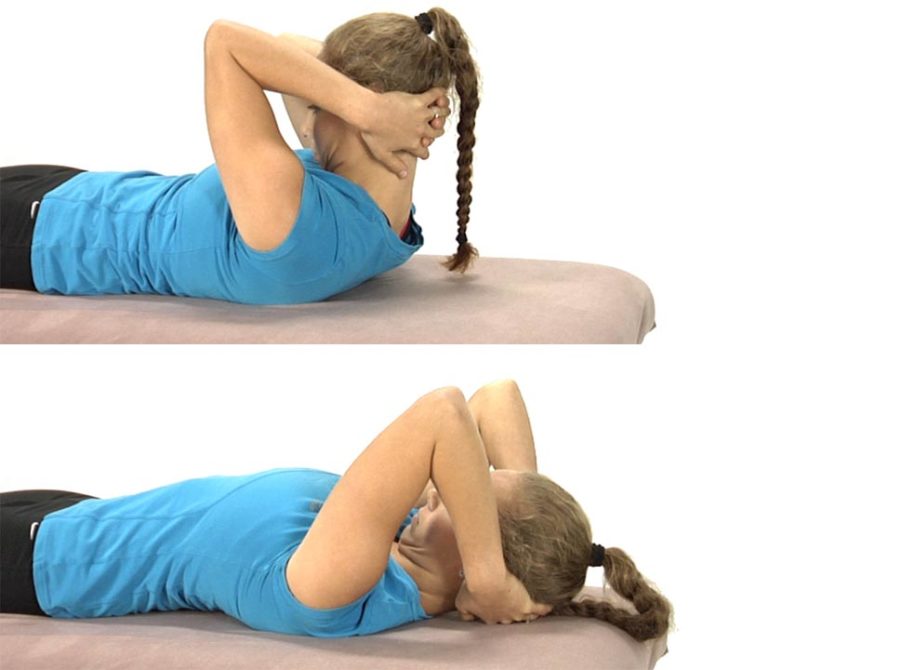
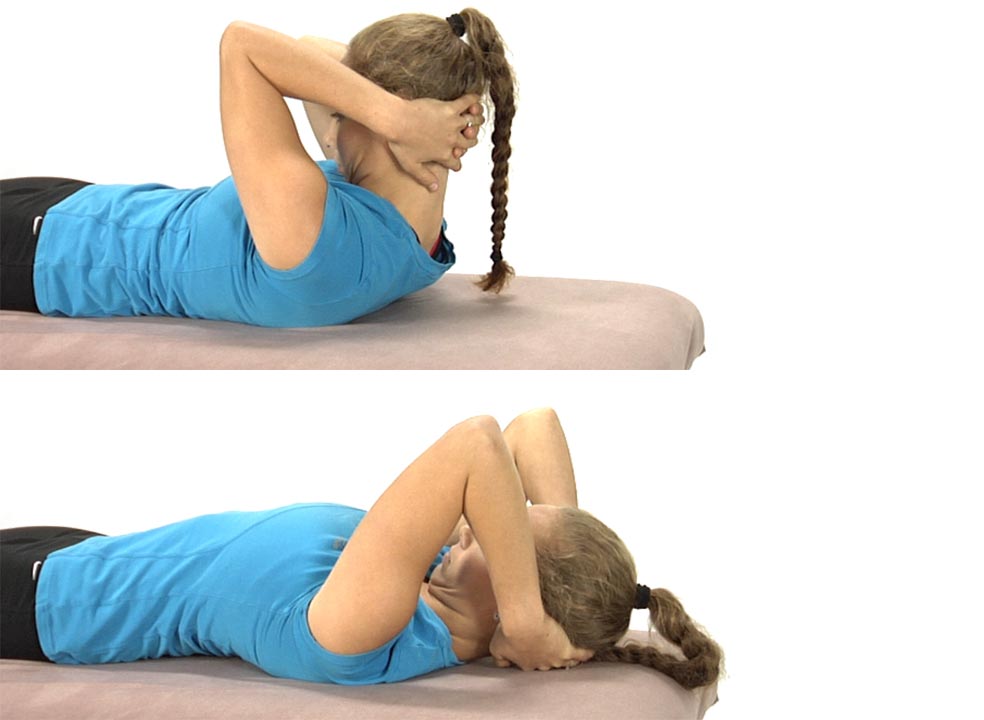
The patient is lying on their back with their hands clasped behind the head.
Instruct the patient to only use their arms to lift their head up so that the chin is drawn toward the chest and a stretch is felt through the back of the neck.
Once the head is brought up fully the patient is told to hold this position for 5-10 seconds, then slowly lower the head back to the table segmentally from below up, using the deep neck flexors eccentrically to lower the head back down to the table and assisting the movement with their hands as needed.
The hands only support the head as needed and an emphasis is placed upon keeping the chin down as the head is returned back to the table.
They repeat 3-5 times.
Eventually as the deep neck flexors become stronger, the hands should no longer be needed to assist in slowly returning the head back to the table.
The goal with this exercise is for the patient to be able to segmentally flex the neck and return back down to the table segmentally without using the hands to assist with the chin staying down throughout the entire movement.
Note: make sure that you can passively flex the patient’s cervical spine in supine lying through its full ROM without feeling any resistance before initiating retraining of the deep neck flexors.
Retraining for this dysfunctional movement test focuses on improving the patient’s sensory awareness and ability to activate the deep neck flexors once the inhibiting factors for recruitment of these muscles has been removed. Therefore the exercises selected will depend upon the ability of the patient to “find” these muscles and recruit them appropriately.
Before attempting to retrain the deep neck flexors the sources of abnormal afferent input need to be addressed first. To review these sources and the recommended treatments see Module 6.