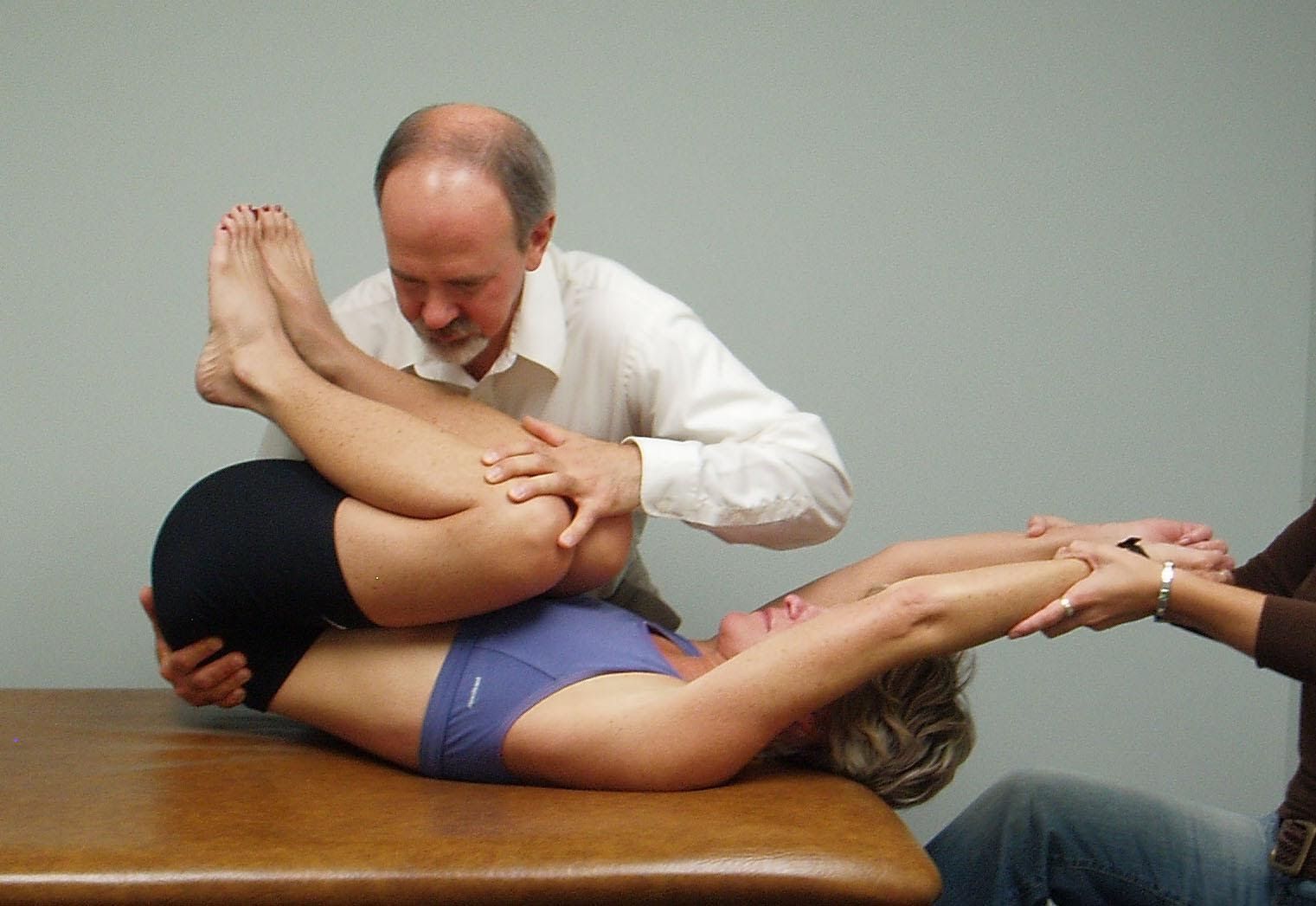
Posterior Capsule Tightness Confirmed by a Loss of Internal Rotation
To confirm tightness in the posterior capsule the patient is placed in ¾ side lying so that the scapula is stabilized against the table
The shoulder is abducted to 90 degrees then IR is introduced
The therapist makes sure that the shoulder stays flat on the table as the arm is passively internally rotated
Normally the patient’s fingertips should comfortably reach the table top (70 degrees of IR)
The test is repeated to both sides for comparison
Note a limitation for IR on the right side in this patient who presented with posterior capsular tightness on the R side
Note: It is extremely important that the therapist is able to differentiate between tightness of the pectoralis minor versus a tight posterior capsule as their treatments are very different. If a patient with a tight posterior shoulder capsule is given a pec minor stretch the patient’s condition can be made much worse.
To Evaluate for Pectoralis Minor Tightness on the R Side
The therapist places their L thenar eminence on the superior border of the patient’s R 3rd thru 5th ribs.
The therapist’s R arm passively raises and supports the patient’s R arm overhead.
The therapist applies an inferior and medial glide to the ribs and pectoral fascia from ribs #3-5 to assess for hypertonicity in the pectoralis minor.
No restriction was detected in this patient who presented with a protracted R shoulder.
Significance of Posterior Capsule Tightness:
Tightness of the posterior capsule correlates to a loss of internal rotation and increased anterior humeral head translation (Tyler et al, 1999; Tyler et al., 2000)
Tightness of the posterior capsule is linked to increased superior migration of the humeral head (Harryman et al., 1990))
A positive Tyler posterior shoulder tightness test has been found in patients with subacromial impingement (Tyler et al, 2000)
Restricted Posterior Capsule and Restricted Shoulder Circles and Hypertonic Pectoralis Minor
Hypertonicity of the pectoralis minor, tightness in the posterior capsule of the shoulder and restricted shoulder circles are addressed together as each type of dysfunction is biomechanically related to the other.
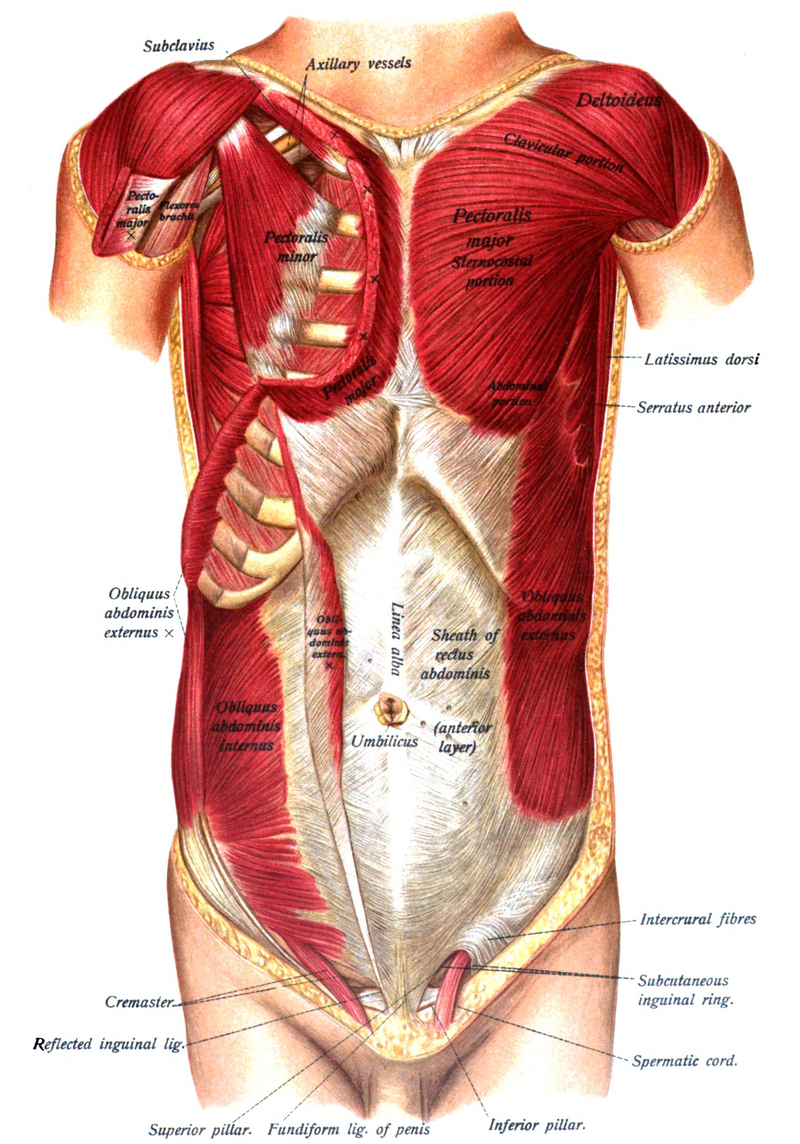
Anatomy and Biomechanical Considerations:
Pectoralis Minor:
Attaches to the superior margins of ribs #3-5 and inserts into the medial aspect of the coracoid process.
Function: With the ribs fixed it anteriorly tilts and IR the scapula
Innervation: Medial pectoral and a branch from the lateral pectoral nerves – C(6),7,8,T1
The patient is kneeling with their elbows on top of a bench or chair and their hips and knees flexed to approximately 90º.
Instruct the patient to place their hands and forearms together and rest their head on their upper arms.
Ask the patient to press the inner borders of their arms together to separate the shoulder blades in back.
Ask the patient to drop their chest toward the floor as much as possible, then perform a posterior tilt (12:00) of the pelvis without lifting up the chest. They should feel a good stretch along the sides, around their shoulder blades.
Have the patient hold the stretch for 30 seconds, then relax and sag the chest further toward the floor. They repeat the stretch 2-3 times.
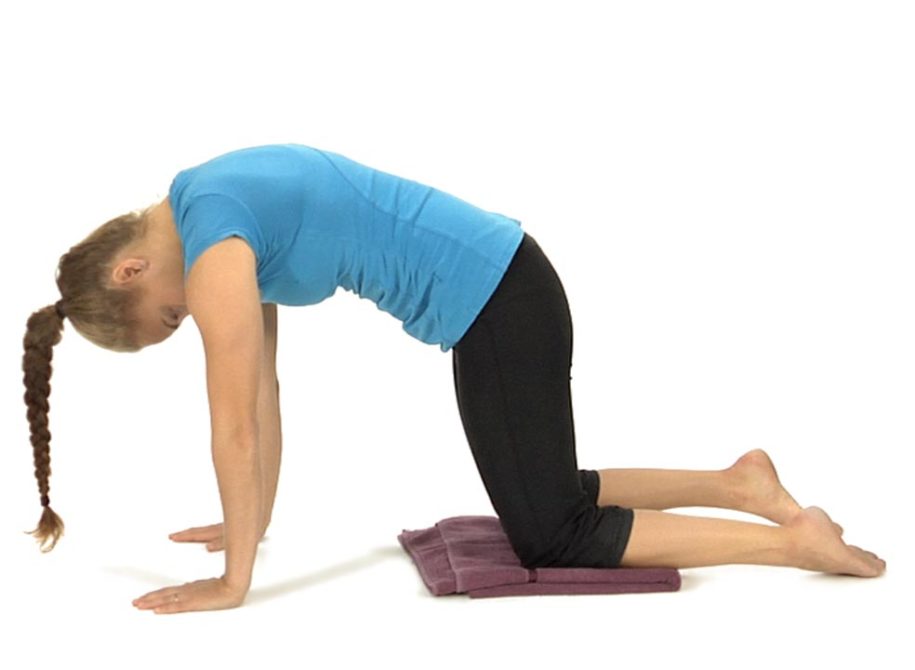
Segmental Cat Backs – Self-Mobilization for Thoracic Extension
The patient is in the hands and knees position with the hands directly beneath the shoulders and knees directly under the hips.
The patient is instructed to drop the head down and segmentally lift their spine towards the ceiling progressing segmentally from the neck then thorax and finally the lumbar spine, finishing by tucking the pelvis under with a posterior tilt.
From this fully flexed position the patient has the option to reverse their spine from the bottom up or from the top down.
If reversing from the bottom up the patient is instructed to anteriorly tilt the pelvis and drop the lumbar spine into lordosis, segmentally progressing up into the thoracic spine with the shoulder blades approximating as the chest drops forward and the neck and head are extended. The therapist observes the motion to make sure that the patient does not skip over a portion of the spine, but moves segmentally as much as possible.
If reversing from above down from the fully flexed position the patient is instructed to lift up their head, extend the neck and drop their chest towards the table with the scapula approximating as the mid-thoracic spine extends. As the motion approaches the lumbar spine the patient drops their belly and anteriorly rotates the pelvis, lifting the tailbone up.
The therapist evaluates in which direction that the patient appears to have better control, from the bottom up or from the top down, and instructs the patient to always initially start the exercise moving in the direction that they have the best control.
The patient repeats the movements 5 to 6 times alternating the initiation of movement from the head and from the tailbone.
Mobilization of the Thoracic Spine in the Lat Dorsi Stretch Position
In kneeling, have the patient place their elbows on top of a bench or chair and walk their knees back until their hips are flexed to approximately 90º.
Their hands and forearms should be together with the head resting on their upper arms.
Ask the patient to press the inner border of their arms together to separate the shoulder blades in back.
The patient is instructed to drop their chest toward the floor as much as possible, then perform a posterior tilt (12:00) of the pelvis without lifting up the chest. They should feel a good stretch along the sides, around their shoulder blades.
The therapist can then apply a posterior to anterior mobilization glide on the spinous process or transverse processes of any segment that appears to be restricted for extension while the patient maintains the stretch or the therapist can perform a myofascial stretch using the fists to draw the soft tissues towards the midline.
The goal is to increase extension in the mid to lower thoracic spine before instructing the patient in self-stretching of the latissimus dorsi.
Remember that the lower trapezius not only contributes to mobility of the shoulder, but is also a thoracic spinal extensor. Consequently studies have found that both mobilization and manipulation techniques to increase extension in the thoracic spine result in an increase in lower trapezius muscle strength, at least in the short term (Liebler et al., 2001 and Cleland et al., 2004).
Dysfunctional Scapular Depression and Shoulder Flexion Tests
Anatomy and Biomechanical Considerations:
The scapular depression tests are used to evaluate the strength/tone of the lower trapezius muscle. The lower trapezius works together with the serratus anterior in a force couple that results in upward rotation, posterior tilt and external rotation of the scapula that is required during elevation of the arm. Note that the lower trapezius is also an extensor of the lower thoracic spine so with restricted thoracic spinal extension (FRS dysfunctions from T6-10) the lower trapezius is inhibited. When the lower trapezius is inhibited the patient may substitute by using the latissimus dorsi to depress the shoulder resulting in downward rotation of the scapula and limited external rotation of the humerus. In addition, hypertonicity in the latissimus dorsi contributes to increasing the thoracic kyphosis and the lumbar lordosis. The bilateral shoulder flexion test in supine allows us to evaluate the length of the latissimus dorsi as well as observe that when it’s hypertonic the patient will compensate by arching the lower back as the latissimus dorsi reaches its end range.
Therefore before attempting to retrain the lower trapezius we must assess for and treat any FRS Dysfunctions from T6-10 and lengthen the latissimus dorsi.
Lower Trapezius:
Attaches to the spinous processes and the interspinous ligaments from T4-T12 and along the medial border of the scapula and medial end of the spine of the scapula.
Function: It upwardly rotates, posteriorly tilts and externally rotates the scapula and assists in extending the thoracic spine from T4-T12.
Innervation: Spinal Accessory Nerve Cranial XI and the dorsal rami from T4-T12.
Inhibited by FRS Dysfunctions from T6-T12.
Latissimus Dorsi:
Attached to the lower 6 thoracic spinous processes and all the lumbar vertebrae, sacrum, crest of ilium and lower 3-4 ribs
Function: adduction and internal rotation of the shoulder, depression of the scapula; extension of lumbar spine and anterior tilt of the pelvis
The scapular stabilization tests are designed to assess the ability of the serratus anterior to hold the medial border of the scapula firmly against the thorax when loading is applied through the arms. If the therapist observes winging of the scapula with either one of these tests then the assumption is that the serratus anterior is weak/inhibited. Often when this occurs you’ll notice that the normal thoracic kyphosis is reduced with straightening of the upper thoracic spine. In extreme cases the upper thoracic spine appears lordotic. Multiple ERS dysfunctions from T3-5 are often found when this has occurred and they need to be addressed first before attempting to retrain and strengthen the serratus.
Anatomy and Biomechanical Considerations:
Serratus Anterior
Attaches from along the medial border of the scapula and especially to the inferior angle, to ribs 1-8 or 9
Functions: upwardly rotates, posteriorly tilts and externally rotates the scapula; protracts the shoulder or posteriorly translates the thorax resulting in flexion of the thoracic spine