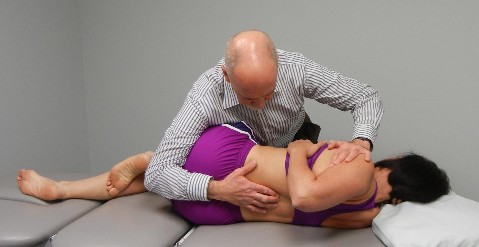
Soft Tissue Mobilization of the Posterior Hip Capsule
Patient is side lying with the treatment side up. The therapist uses the elbow to scour around the posterior aspect of the hip capsule feeling for areas of tension. The therapist can also work from the posterior aspect of the greater trochanter back across the gluteal area to the sacrum and address any tension in the external rotators of the hip with deep friction massage.
Passive Mobility Testing in Extension with Translation of the Shoulders from Right to Left to Detect FRS R Dysfunctions
Patient is prone propped on elbows with their elbows together and hands under their chin.
Place your right thumb on the left side of the SP and rest your left forearm over the patient’s shoulders.
Translate the patient’s shoulders from right to left as you block the SP and assess for tightness. Repeat from T10 to L3
With an FRS R dysfunction you’ll feel a blockage when attempting to draw the spine over your stabilizing L thumb
FRS dysfunctions are commonly found with this test anywhere from T11- L2 resulting in a positive FADIR test that is perceived as a tight posterior hip capsule
Patient is seated and asked to cross one leg over the other. Notice the limitation on the patient’s right side when compared to the left side. Remember that the piriformis is an internal rotator of the hip above 60 degrees of hip flexion.
Operator palpates under the twelve rib for hypertonicity in the quadratus lumborum muscle
Hypertonicity in the quadratus lumborum on one side is associated with a FRS dyfunction at the TL junction on that side, i.e., hypertonic right QL found with an FRSR at T12-L1
Dysfunctional Trunk Rotation and/or Dysfunctional Hip Abduction Functional Movement Tests
These dysfunctional movement tests can be best addressed by mobilizing any spinal dysfunctions that are found at the thoracolumbar junction and/or by stretching the quadratus lumborum and piriformis muscles. It is also sometimes helpful to mobilize the inferiomedial hip capsule and stretch the hip adductors as covered in 4b. These sources of inhibition should be addressed before attempting retraining.
Anatomy and Biomechanical Considerations:
Quadratus Lumborum, Piriformis and Posterior Hip Capsule
Observations:
Hypertonicity in the quadratus lumborum on one side is associated with a FRS dysfunction at the TL junction on that side, i.e., hypertonic right QL found with an FRS R at T12-L1.
Pinching in the anterior groin with FADIR test or when attempting to stretch the piriformis is related to a tight posterior hip capsule. “Groin pain is posterior hip capsule tightness until proven otherwise”, Dr. Philip Greenman.
An apparent tightness in the posterior hip capsule dissipates, often times dramatically, after mobilizing the upper lumbar spine for FRS dysfunctions on the same side, ie., tight R posterior hip capsule, FRS R at L1,2 or L2,3 will be present.
Therefore, before we treat the quadratus lumborum, piriformis and posterior hip capsule we need to first identify and treat any FRS dysfunctions found between T12-L2.
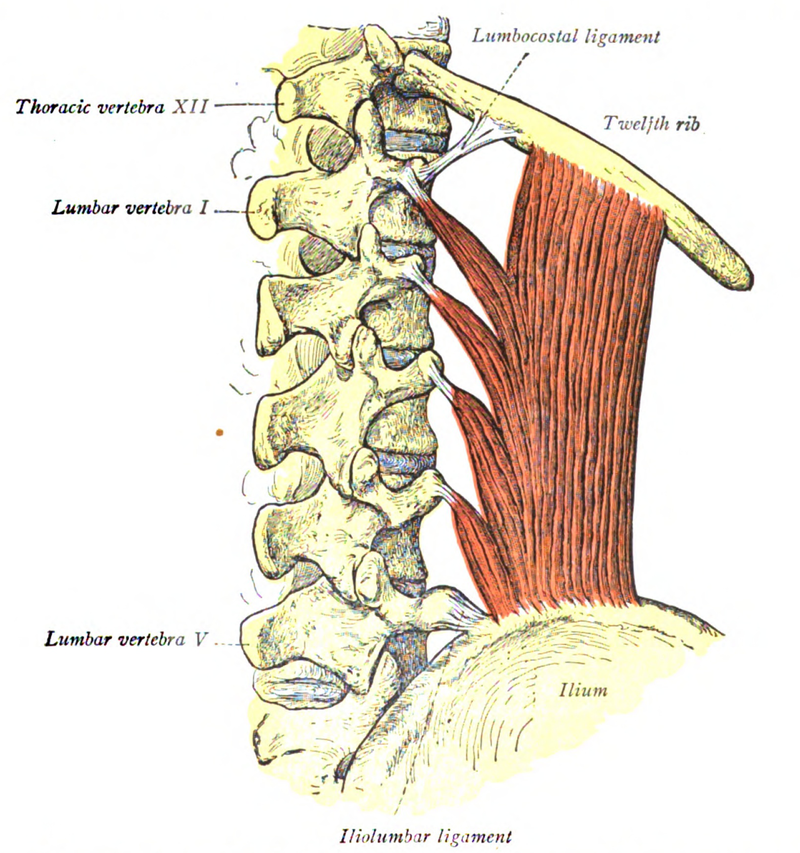
Quadratus Lumborum
Three distinct divisions:
Lateral (global mobilizer)
Iliolumbar
Lumbocostal
Function – stabilizer of the lumbar supine, a lateral flexor of the lumbar spine and a hip hiker
Innervation – thoraco-lumbar spinal nerves
Most frequent muscular cause of back pain (Travell and Simons, 1992)
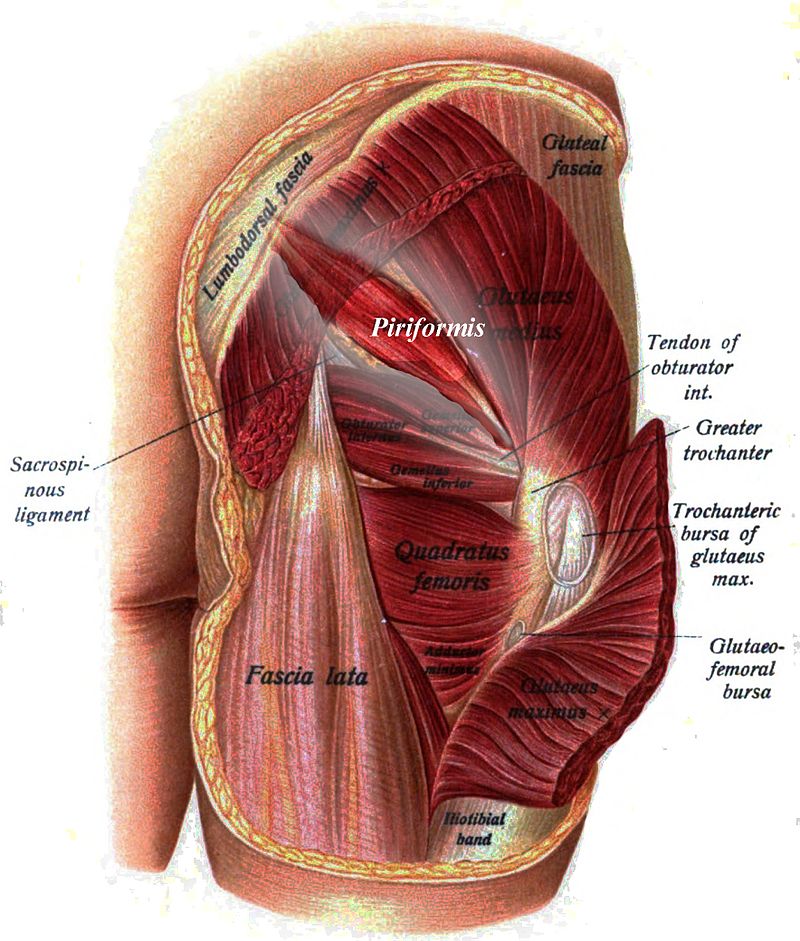
PIRIFORMIS: Origin at S 2-4, exits to insert at greater trochanter.
It crosses the SI joint and hypothetically influences the oblique axis of the sacrum during coupled motion.
Attaches to the anterior surface of S2, 3, 4 and inserts into the greater trochanter
Below 90º of hip flexion it abducts and ER the hip
Above 90º of hip flexion it abducts and IR the hip
Innervation – S1 and 2
FIVE EXTERNAL ROTATORS OF HIP Obturator internus Obturator externus Gemellus superior Gemellus inferior Quadratus femoris
(These muscles are intimately attached to the posterior hip capsule.)
Patient is lying on their left side with a pillow under the head and the shoulder and hips perpendicular to the table.
The hips are flexed to approximately 45º with the knees flexed and the feet touching.
Ask the patient to slowly raise the right knee as high as possible keeping the feet in contact.
Compare the right to the left side, and compare any limitations noted in range of motion with the degree of inhibition of the gluteus medius on that side.