The patient is lying on their back and places one hand under the upper part of the neck, at the base of the skull.
Ask the patient to attempt to nod the chin down slightly, increasing the pressure against the hand under the upper neck. Instruct the patient to avoid pushing their head back toward the table.
There should not be any palpable tension in the superficial muscles in the front of the neck as they perform the exercise.
The patient is instructed to hold for 10 seconds and repeat 3-5 times, gradually working up to 10 repetitions.
In sitting, instruct the patient to palpate the muscles in the front of the neck.
Then instruct the patient in using the deep neck flexors by nodding their chin down slightly towards their chest. Explain to the patient to try to avoid activating the superficial muscles that their are feeling in the front of the neck.
Emphasize tucking the chin toward the chest rather than bending the head forward. Little actual movement of the head should occur if done correctly.
The patient may feel a slight stretch at the base of their head.
For an ERS Left and or high tone in the Left Erector Spinae:
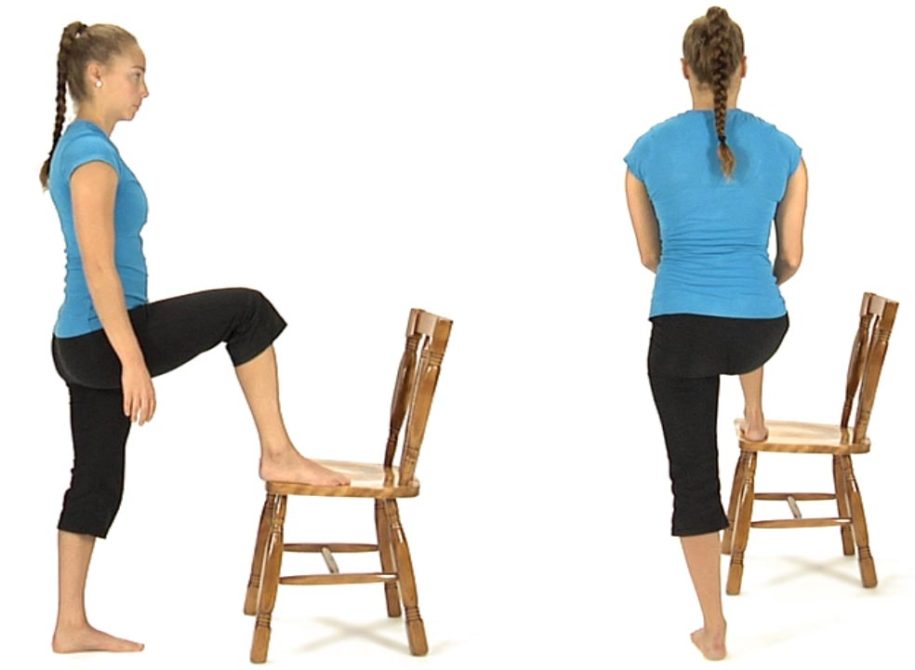
The patient starts in standing and places their right foot up on a chair.
Instruct the patient to place their hands around each side of their right knee and slide their hands down the leg towards the ankle attempting to bring the chest down towards the right knee.
They hold the stretch for 5 to 10 seconds then return to upright standing.
Have the patient repeat this sequence 8 to 10 times.
For an ERS Right they place the left foot up on a chair.
To treat an ERS Right and/or high tone in the Right Erector Spinae:
The patient starts this exercise in the hands and knees position and is instructed to sit back diagonally as though attempting to sit onto their right hip.
Instruct the patient to sit back as far as they can without holding onto the table with their hands.
Have them hold the position for 5 seconds then come back up to the original hands and knees position without pulling up with their arms.
Muscle Energy Technique: ERS Dysfunction in the Lower Thoracic Spine
The therapist places their L index and middle fingers on the L side of the spinous processes and translates the spine towards him looking for any restriction in L to R translation (L side bending). If the restriction is worse in flexion and improves in extension the diagnosis is an ERS R.
To treat the ERS R the therapist has the patient sit up tall initially, then introduces flexion from above down and below up creating an apex for flexion at the palpated segment. L side bending is then introduced by translating the patient’s shoulders from L to R to the feather edge of the L side bending barrier. The patient is instructed to gently side bend to the R for 5-7 seconds and then relax.
The therapist takes up the slack by further translating the shoulders to the R. This is repeated 3-4 times.
Dysfunctional Supine Curl Up Functional Movement Test
This dysfunctional movement test can be best addressed by first mobilizing any ERS spinal dysfunctions that are found in the lower thoracic spine and thoracolumbar junction that restrict spinal flexion followed by stretching the erector spinae muscles. These inhibitory influences should be addressed before attempting to retrain this dysfunctional test.
It is also sometimes helpful to stretch the hip flexors as covered in #3b and c.
Anatomy and Biomechanical Considerations:
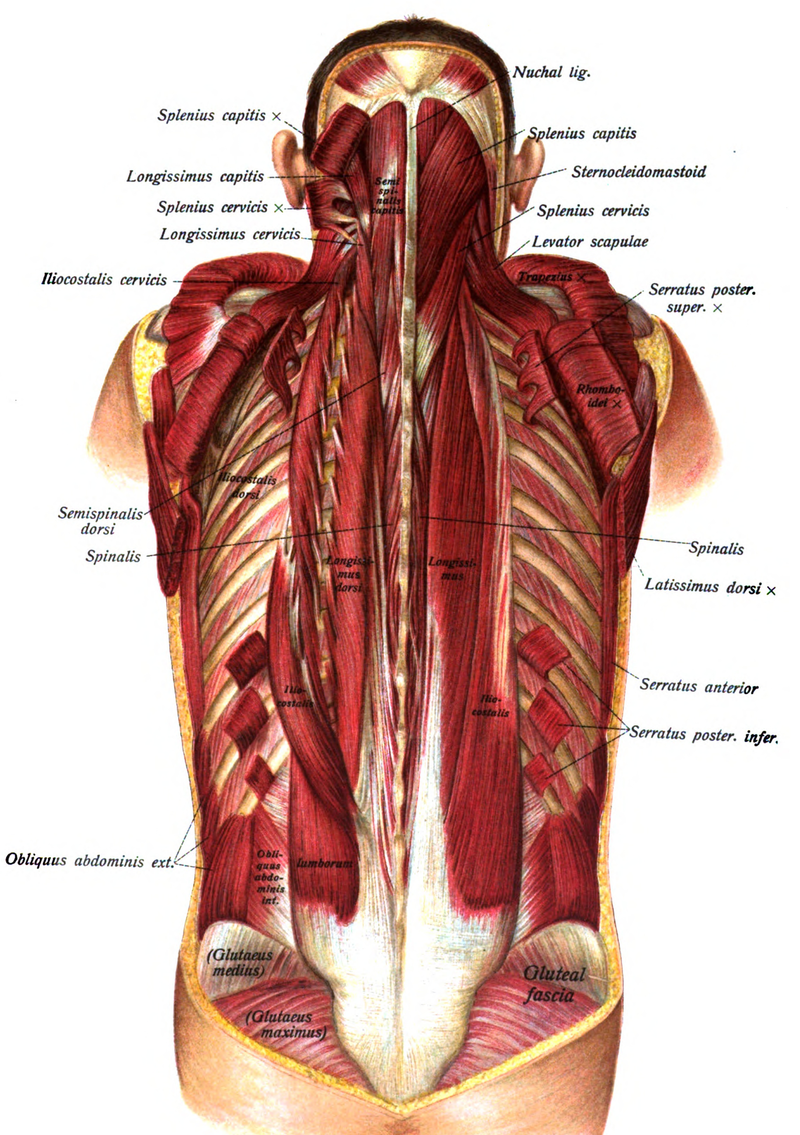
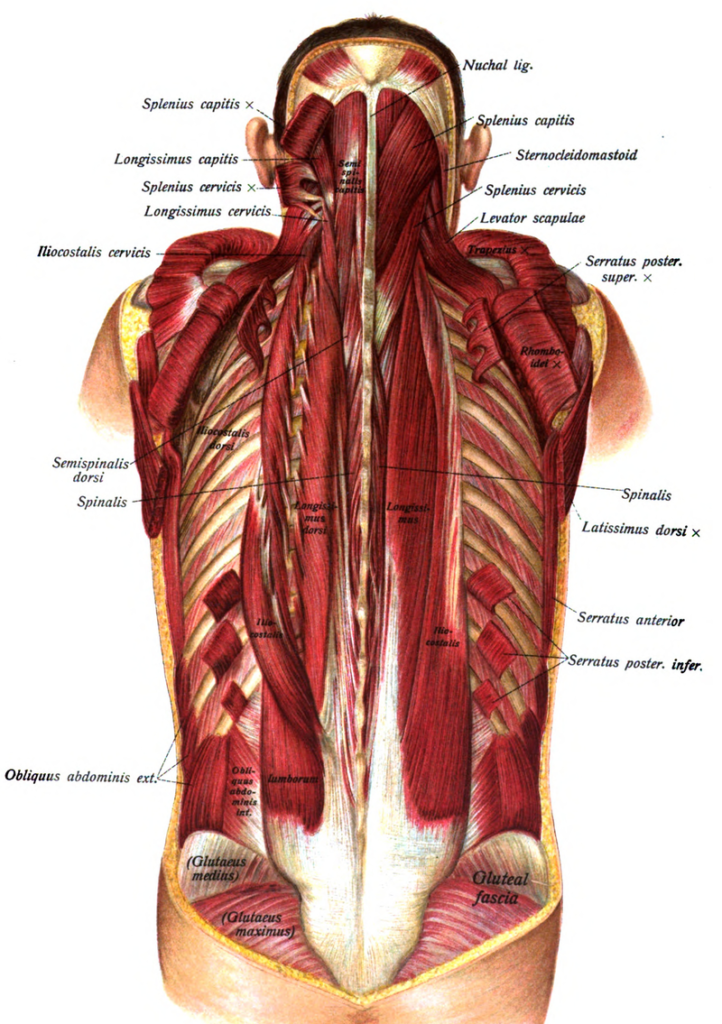
The erector spinae muscles consist of the longissimus thoracis and iliocostalis thoracis and iliocostalis lumborum muscles. These muscles working unilaterally rotate the spine to the ipsilateral side and when working bilaterally they extend the spine. The longissimus thoracis muscle becomes hypertonic when there is a non-neutral dysfunction in the thoracic spine. This hypertonicity, which is often seen unilaterally, results in inhibition of the abdominals and interferes with the ability to perform a curl up and/or reverse the lumbar lordosis during forward flexion.
Dysfunctional Hip Abduction and ER and/or Dysfunctional Hip Abduction Functional Movement Tests
These dysfunctional movement tests are best addressed by mobilizing the inferiomedial hip capsule, stretching the hip adductors and/or obturator nerve, and mobilizing the sacral base to restore restricted anterior nutation on the dysfunctional test side before retraining is initiated. Also a pubic symphysis dysfunction needs to be addressed, if present, as it represents an imbalance in tone between the hip adductors and abdominals and can contribute to, or be the source of these dysfunctional movement tests.
Mobilizing the hip in an inferiomedial direction in side lying at 45 degrees of passive hip abduction has been shown to improve isometric torque in the hip abductors, in the short term, in healthy subjects. (Makofsky et al., 2007). This response is proposed to be due to a reduction of an inhibitory and dysfunctional arthrokinetic reflex from a tight inferiomedial joint capsule (Warmerdam, 1999).
Anatomy and Biomechanical Considerations:
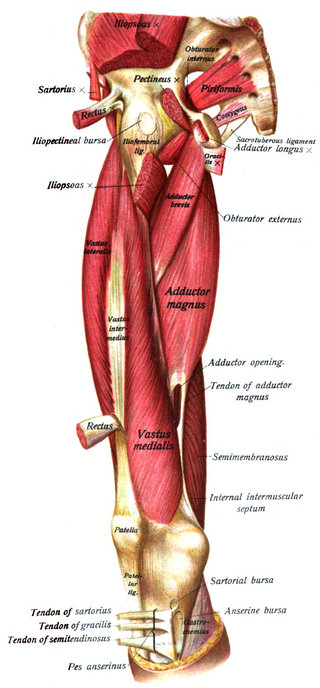
Hip Adductors
Attach to the pubic ramus and ischial ramus to ischial tuberosity
Function to restrain abduction of the stance limb during gait
They also assist in internal rotation and flexion of the hip
Hypertonicity of the hip adductors can result in displacement of the femoral head superiorly and laterally
Innervation – obturator n. L2, 3 and 4
Anterior Oblique Sling
Adductors are functionally connected to the abdominal obliques on the contralateral slide to form an oblique sling of support for the anterior pelvis
When hypertonic the pull of the adductors can result in an inferior pubic shear