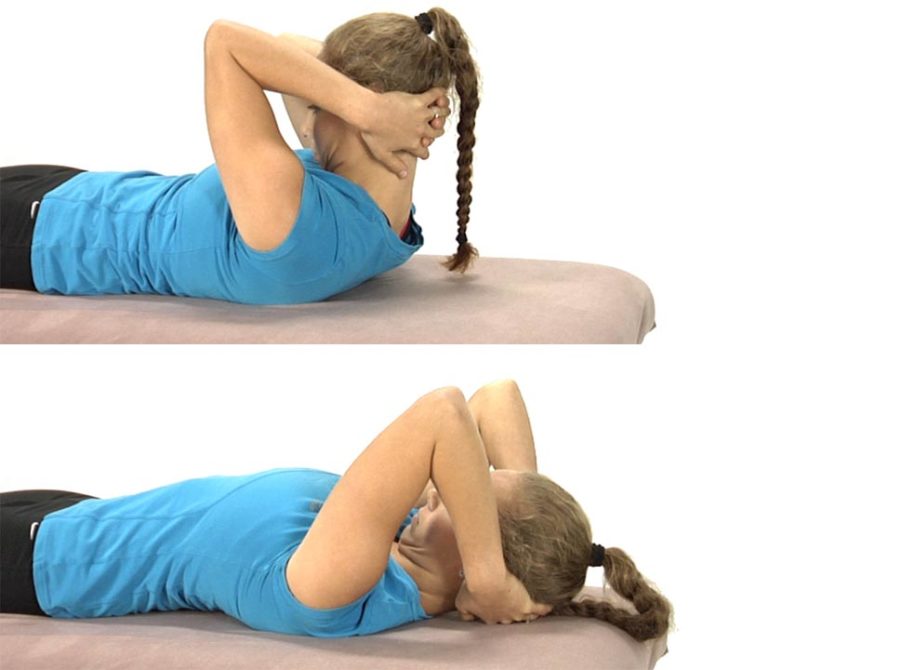
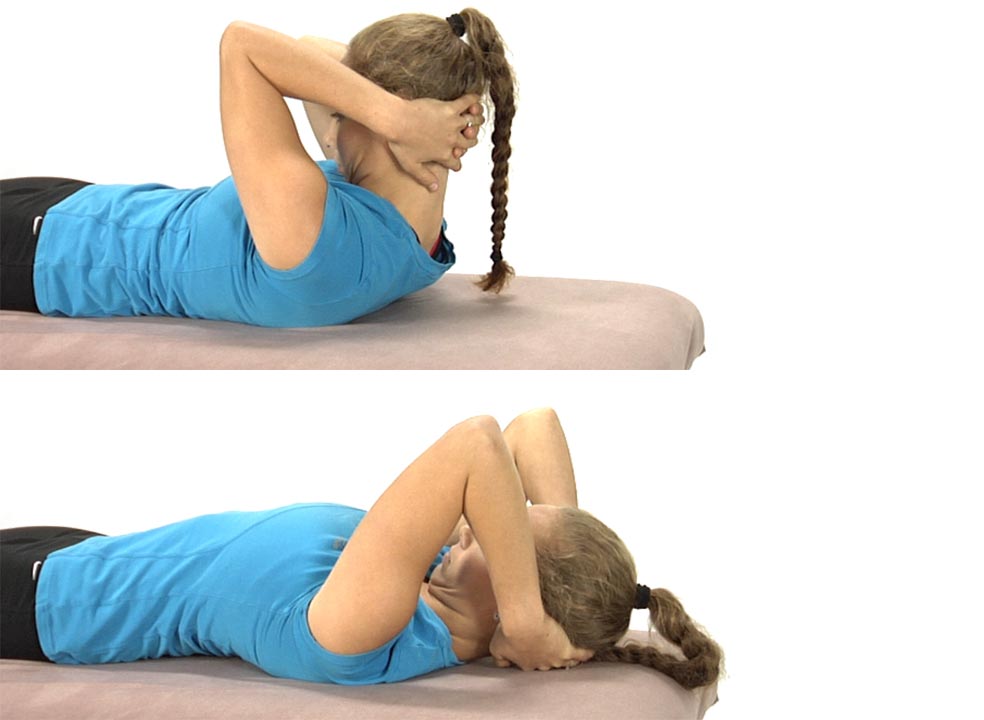
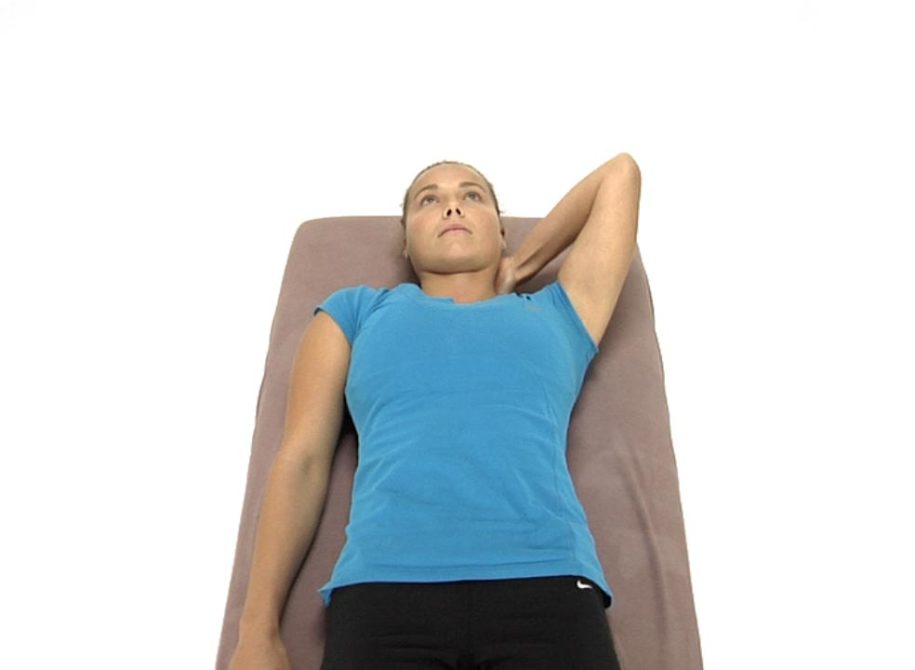
The patient is lying on their back with their hands clasped behind the head.
Instruct the patient to only use their arms to lift their head up so that the chin is drawn toward the chest and a stretch is felt through the back of the neck.
Once the head is brought up fully the patient is told to hold this position for 5-10 seconds, then slowly lower the head back to the table segmentally from below up, using the deep neck flexors eccentrically to lower the head back down to the table and assisting the movement with their hands as needed.
The hands only support the head as needed and an emphasis is placed upon keeping the chin down as the head is returned back to the table.
They repeat 3-5 times.
Eventually as the deep neck flexors become stronger, the hands should no longer be needed to assist in slowly returning the head back to the table.
The goal with this exercise is for the patient to be able to segmentally flex the neck and return back down to the table segmentally without using the hands to assist with the chin staying down throughout the entire movement.
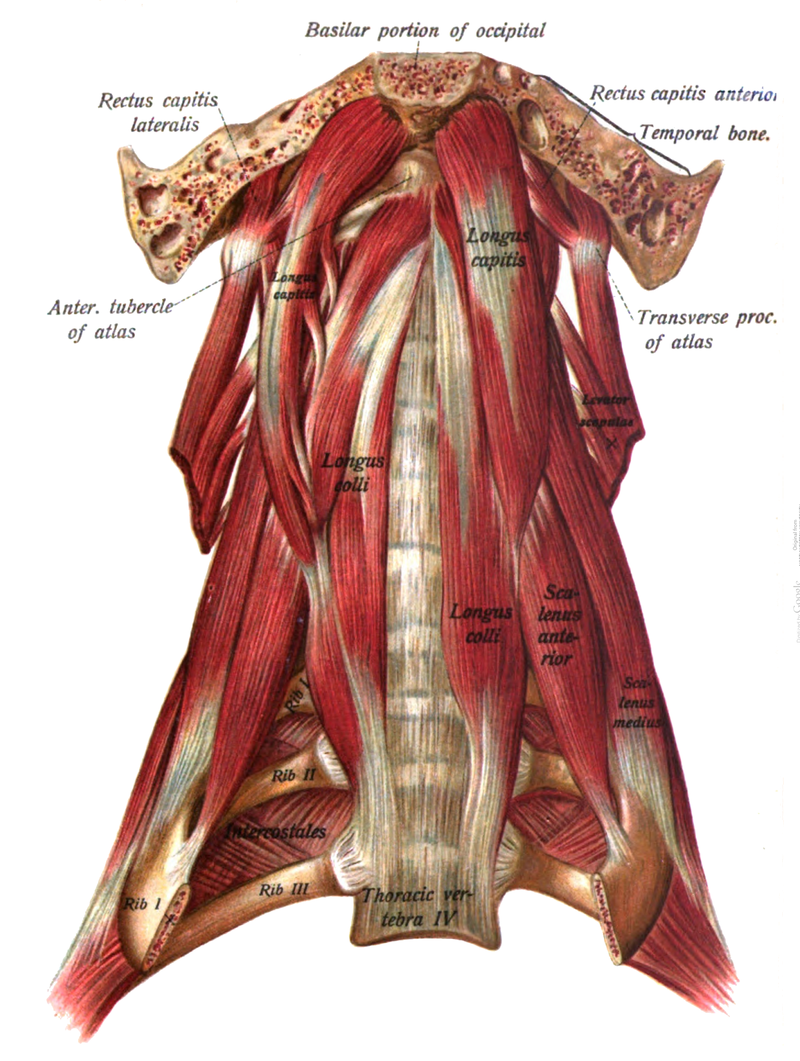
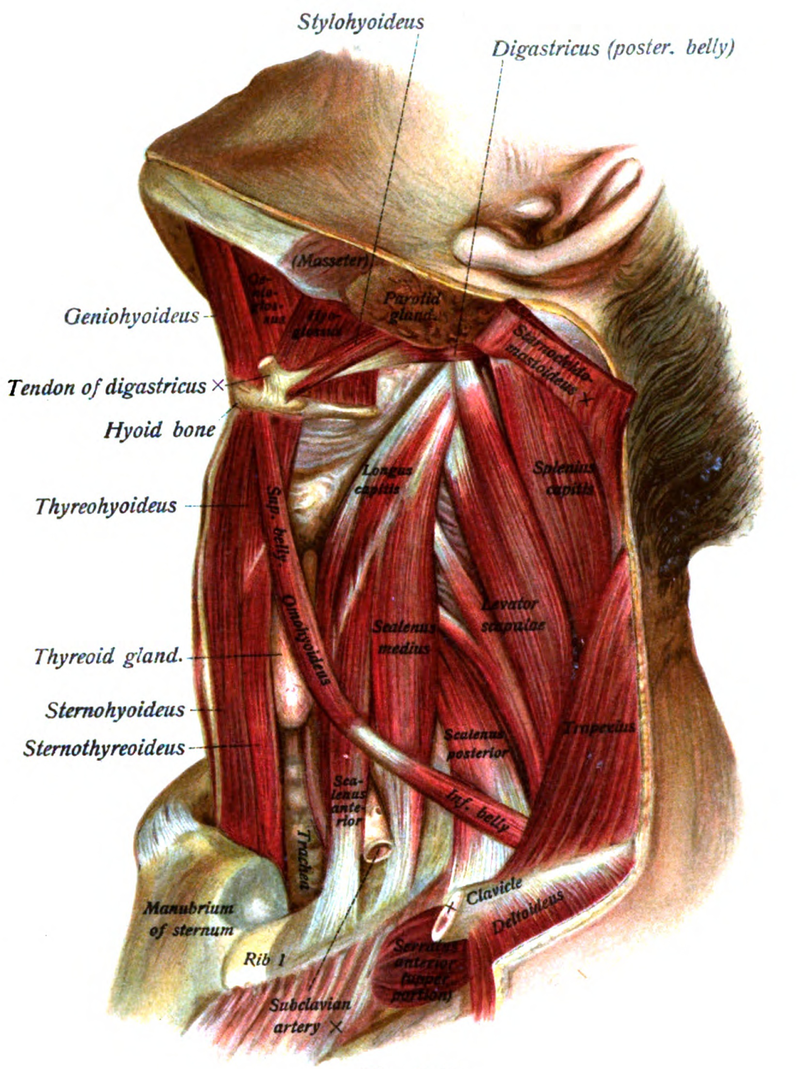
The cervical flexion test assesses the ability of the patient to segmentally flex the cervical spine using the longus colli, longus capitis and rectus capitis anterior assisted by the SCMs, anterior scalenes and infra and suprahyoid muscles. When the primary deep neck flexors are inhibited/weak the SCMs and anterior scalenes substitute for this weakness and become the primary neck flexors resulting in the chin tipping up and the upper CS extending rather than flexing during the performance of this test (Janda, 1994).
Abnormal afferent information that can contribute to this muscle imbalance can occur when ERS dysfunctions of the cervical and especially upper thoracic spine are present. These ERS dysfunctions can result in inhibition of the longus colli and longus capitis due to restricted active and passive ROM for neck flexion. In addition, hypertonicity of the scalenes occurs in apical chest wall breathers as the scalenes, which are normally only accessory muscles recruited with deep inhalation, become recruited with every breath. Palpation of the scalenes in these patients will confirm the recruitment of these muscles even during relaxed breathing. This typically is felt to occur more on the R side than the L. Asking these patients to take a deep breath while the therapist palpates the lower lateral rib cage for normal bucket handle motion will reveal restricted excursion on the R side in these patients.
Self Mobilization for Adverse Neural Tension in the Cervical Spine
To treat the right side of the neck:
The patient is lying on their back and places their left hand under the neck with their fingers wrapping around to the right side of the neck. The therapist instructs the patient as to the specific location for the patient to place their finger contact.
Tell the patient to gently pull their neck to the left using their left hand and hold this position.
The patient’s R arm is down at their side with the palm facing the ceiling.
Have the patient slowly abduct their arm as far as they can without allowing the cervical spine to translate back to the R.
The patient returns the R arm back down to the side and is instructed to take up any slack that they feel for additional R to L translation and repeat again.
The patient repeats the movement 8-10 times holding their neck still and translated to the L as they try to abduct their R arm higher with each successive repetition.
Mobilization of Adverse Neural Tension on the R side of the Cervical Spine
The therapist introduces translation from right to left with his/her contact on the dysfunctional articular pillar.
The patient is instructed to slowly abduct their R arm along the table as far as they can while the therapist maintains the right to left translated position of the cervical spine and prevents the dysfunctional segment from translating back to the right.
This is repeated several times. Each time the patient lowers their arm to their side the therapist takes up any additional slack for right to left translation.
Goals for treatment: translation from right to left at the previously noted dysfunctional segment is now free and the patient should be able to fully and comfortably abduct the right shoulder overhead without the therapist feeling the cervical spine translate to the right at any segmental level.
Assessment and Treatment of Adverse Neural Tension That Occurs During Active Shoulder Abduction
To assess for adverse neural tension on the right side of the neck:
Assess translational mobility of the cervical spine from right to left with your right hand contact on the articular pillars of the cervical spine.
If you find multiple levels are restricted for right to left translation, then translate the level of greatest restriction to the left with your right hand contact on the articular pillar of the cervical vertebrae.
Hold this translation and ask the patient to slowly abduct or slide their right arm up along the table.
Ideally the patient should be able to fully abduct the arm without the therapist feeling the articular pillar pushing back toward the right against their R hand contact.
When there is adverse neural tension in the R brachial plexus the cervical spine will be drawn to the R side by the hypertonic R scalenes and even more so during active R shoulder abduction.
Instruct the patient to sit up tall and place their left hand over the right first rib and clavicle to stabilize. The patient’s right hand grasps the bench or chair to further stabilize the neck.
Keeping their chin down, ask the patient to bring their head straight back into extension, side bend the head to the left and rotate back to the right.
They should feel a stretch through the front of their neck on the right side.
They hold for 30 seconds and repeat 2-3 times.
Then have the patient repeat the stretch on the L side.
Muscle Energy Technique to Stretch the Right Scalenes
The patient’s head and neck, down to T2, are brought off the end of the table and supported by the therapist’s L forearm. The patient is instructed to grasp the table with their right hand to stabilize the first rib.
The therapist grasps the base of the occiput with the left hand and places their left shoulder against the patient’s forehead.
The therapist’s right hand is placed over the top of the patient’s right shoulder to further stabilize the first rib.
The therapist translates the patient’s head straight down towards the floor maintaining upper cervical spine flexion by keeping the patient’s chin down at all times. The therapist then adds side bending of the head to the left and rotation back to the right, maintaining the AP translation.
The patient is asked to take and hold a deep breath and raise the head up against the therapist’s L shoulder for 5 to 7 seconds.
Upon relaxation the therapist takes up the slack by increasing the AP translation, left side bending and right rotation.
This procedure is repeated 3 to 4 times.
Assessment of right to left translation of the typical cervical spine (C3-7) before and after treatment of the right scalenes helps to confirm your success with this treatment.
Treatment of a superiorly subluxed first rib on the left
Patient is seated with the therapist standing behind.
The patient’s right arm rests on top of the therapist’s right leg.
The therapist places the finger pads of the 2nd, 3rd, and 4th fingers anterior to the left trapezius muscle pulling it posteriorly.
The finger pads are placed on top of the left 1st rib.
The therapist’s right hand and forearm control the right side of the patient’s head and neck. The patient’s head is flexed forward down to the level of the first rib.
Left side bending and slight left rotation of the patient’s head and neck are introduced to take the left scalenes off tension.
The therapist’s left thumb applies a firm anteriorly directed force to the posterior aspect of the first rib.
The patient is asked to attempt to side bend the head to the right with exhalation to reciprocally inhibit the left scalenes while the therapist applies a firm counterforce to prohibit the neck from moving.
Following relaxation the therapist repositions the patient’s head into more left side bending all the while maintaining a firm anteriorly directed push on the posterior aspect of the first rib.
After three to four repetitions and after the final contraction and relaxation effort the therapist rotates the patient’s head fully around to the left to take T1 to the left while maintaining the anterior pressure with the left thumb so that the rib can drop down without force.
Three areas of potential compression of the brachial plexus resulting in positive ULTT1 or ULTT3 tests
In the intrascalene triangle
In the costoclavicular space
Underneath the pectoralis minor – hyperabduction syndrome
Intrascalene Triangle:
Hypertonicity of the anterior and middle scalenes
Brachial plexus lies between the scalenes
The brachial plexus and scalenes are both contained in the deep fascia of the cervical spine
Costoclavicular Space
Elevated first rib due to hypertonic scalenes
Superiorly subluxated first rib – confirmed by the cervical rotation/lateral flexion test
Pectoralis Minor – Hyperabduction Syndrome
Compression of the brachial plexus during shoulder abduction secondary to a tight pectoralis minor
Tone of the pectoralis minor is influenced by the position and mobility of ribs 3-5
Factors Influencing the Three Areas of Compression often resulting in a diagnosis of Thoracic Outlet Syndrome:
Hypertonic scalenes
Superiorly subluxated 1st rib
Hypertonic pectoralis minor/hypomobility of ribs 2-5
Superiorly Subluxated First Rib:
Mechanism of injury – acute side bending injury to the neck, ie, broadsided MVA or a strain on the neck when transferring a patient
Diagnosis: Palpation reveals the rib to be elevated by a thumb’s width compared to the other side
Positive Cervical Rotation/Lateral Flexion (CRLF) Test
Positive Adverse Neural Tension signs
Diagnosis of Thoracic Outlet Syndrome
Palpation for a Superiorly Subluxed First Rib (Lindgren, Leino, Manninen, 1992):
Illustration of a superiorly subluxated first rib on the left – the rib must be at least a finger width’s difference in height to make the diagnosis.
Compare this palpation test with the cervical rotation lateral flexion (CRLF) test.
To perform the CRLF test the patient is either sitting or supine and the neck is passively rotated to the left then laterally flexed to bring the right ear towards the chest. This tests the right first rib. The test is then repeated on the opposite side for comparison.
Cervical Rotation/Lateral Flexion Test (CRLF) to Diagnose a Superiorly Subluxated First Rib:
To test for a superiorly subluxated first rib on the right: Therapist passively rotates the patient’s head to the left then attempts to laterally flex the head to the right bringing the right ear towards the chest.
A comparison is made with the opposite side. A positive test is indicated when the range of lateral flexion is reduced and a bony or hard end feel is felt by the therapist when the transverse process of C7 contacts the superiorly elevated rib.