Cervical Flexion Test
How to Perform
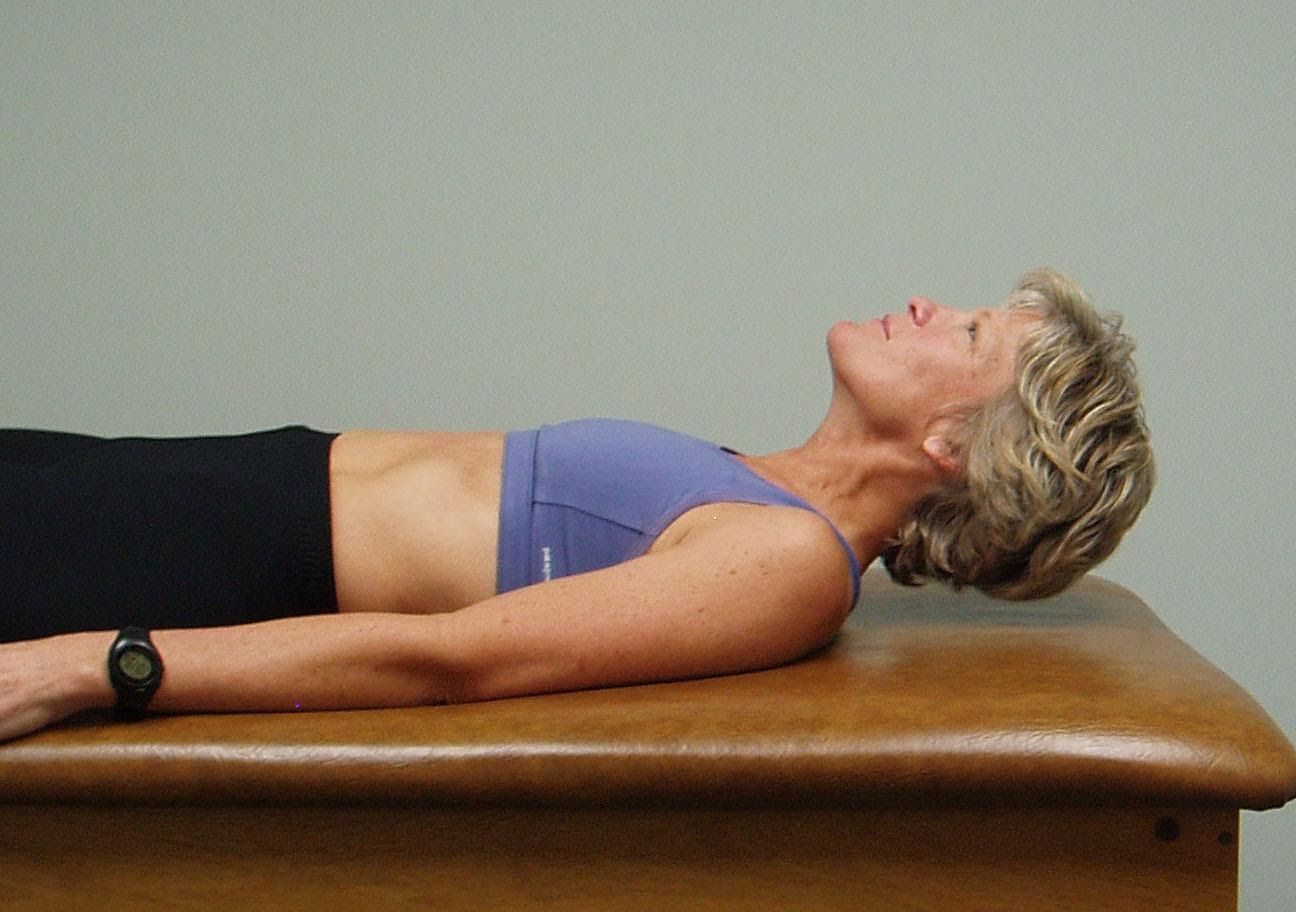
- The patient is supine with legs straight and arms down to the sides.
- Ask the patient to raise the head off the table and look down towards their feet.
- Observe how the patient lifts the head, does the patient initiate the movement by progressive segmental flexion from above down or do they initiate the movement leading with the chin up?
Interpretation and the most common dysfunctional pattern seen
Normally the patient should be able to easily lift up their head and segmental flex thru the cervical spine utilizing their deep neck flexors throughout the full range of motion (pictured on the top)
The therapist watches for the chin to protrude forward indicating substitution by the sternocleidomastoid muscles for the inhibited deep neck flexors (pictured on the bottom).
If this movement is viewed as dysfunctional the therapist should then passively flex the neck to determine if this is a mobility problem or an inhibition problem. If passive ROM is restricted this is a mobility problem due to tight cervical extensors, an ERS dysfunction of the upper thoracic spine, hypertonic upper trapezius and/or levator scapulae, adverse neural tension, etc. If passive ROM of the cervical spine is free, but the active movement is dysfunctional think about a motor control/inhibition problem.