Dysfunctional Cervical Flexion Test
Barry Wyke, 1981 reported that when experiencing pain in the neck and/or low back there is facilitation of the spinal extensors and inhibition of the spinal flexors. In describing muscle imbalances found in his Upper Crossed Syndrome Janda (1994)) observed that the neck extensors are tight (SCM and suboccipitals) and the deep neck flexors are inhibited and weak.
Jull (1994 and 1997) studied the recruitment of the deep upper cervical flexors in patients with neck pain using a biofeedback cuff placed under the upper cervical spine that they used to measure the amount of pressure a patient can produce when asked to perform upper cervical flexion without recruiting the superficial neck flexors. Patients with neck pain were found to display a deficit in their ability to activate and maintain contraction of the deep neck flexors.
If the cervical flexion test is dysfunctional you first need to determine if there is also a restriction for passive cervical flexion. Restricted passive cervical spine flexion indicates a mobility problem that needs to be addressed first before attempting to retrain the deep neck flexors. Restricted passive neck flexion can be due to the presence of ERS dysfunctions in the upper thoracic and lower cervical spine, hypertonicity of the levator scapula and splenius cervicis muscles or as a consequence of adverse neural tension. Once passive supine cervical flexion mobility is free then retraining as presented in Module #7 can begin.
Anatomy and Biomechanical Considerations:
Cervical flexion requires that the cervical and upper thoracic facet joints can bilaterally open and slide superiorly freely. The cervical flexion test if done sequentially from above down requires that the chin approaches the chest and remains there through the full range of neck flexion. Remember that the SCM muscles when activated bilaterally, participate in flexion of the typical cervical spine, but extension of the upper cervical spine. It is because of this dual action of the SCMs that with inhibition of the deep neck flexors we see patients extend the upper cervical spine during the cervical flexion test leading with their chin up.
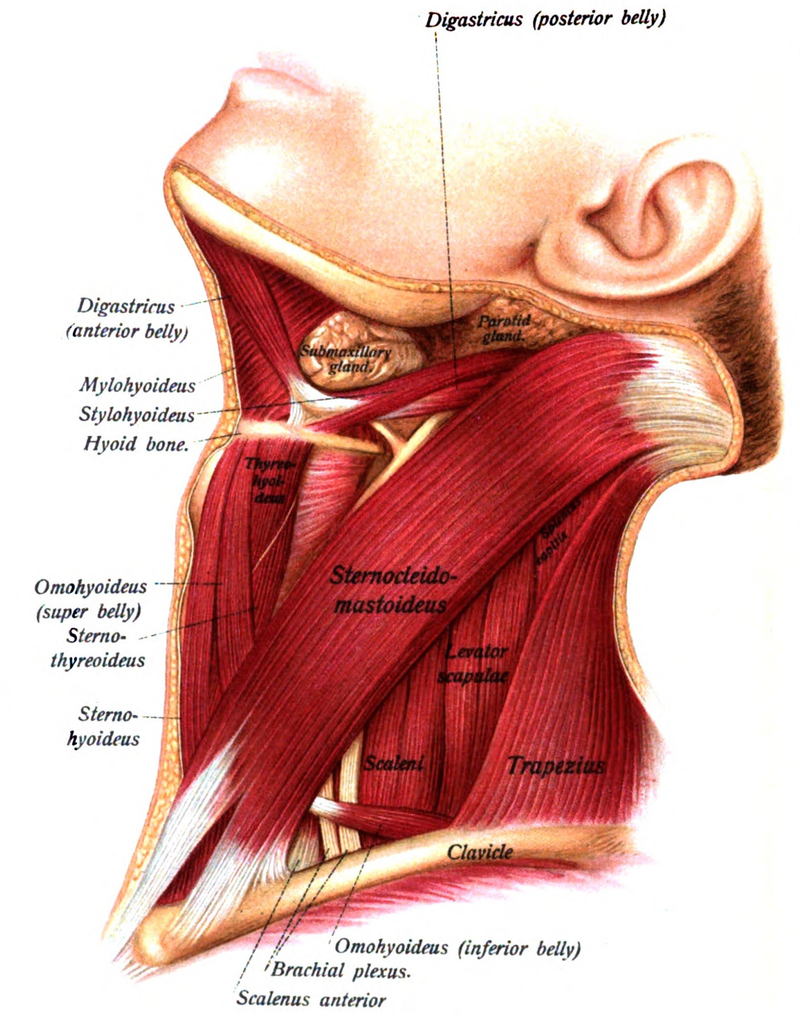
Sternocleidomastoid:
- Two divisions: sternal and clavicular attach into the mastoid process of the temporal bone
- Function: bilateral activation – flexion of the typical CS and extension of OA, unilateral – side bends to the same side and rotates to opposite side
- Innervation – spinal accessory n., cranial XI
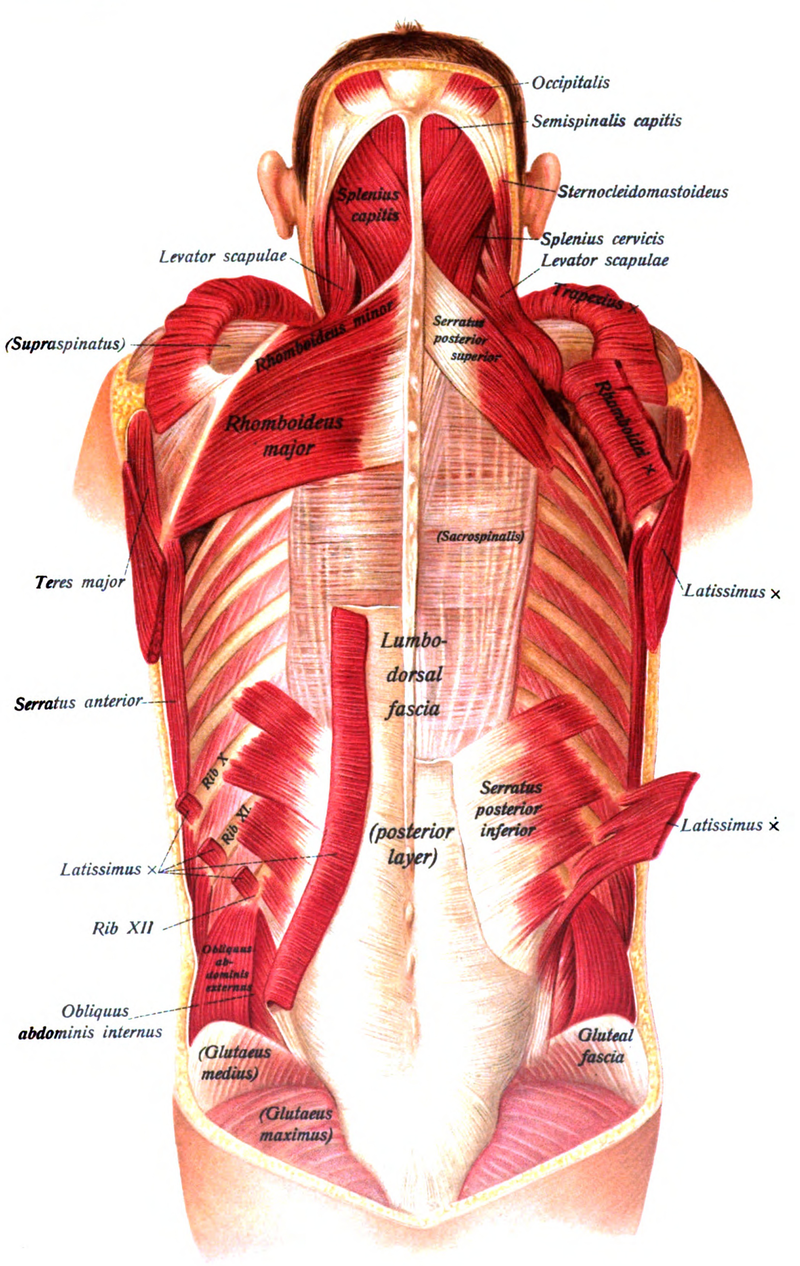
Levator Scapulae and Splenius Cervicis:
The levator scapulae attaches from C1-C4 and with the scapula fixed, extends, side bends and rotates the cervical spine to the ipsilateral side
When hypertonic these muscles not only restrict passive neck flexion, but also they can act as long restrictors at multiple levels of the cervical spine for passive translation to the contralateral side when the spine is tested in flexion