Dysfunctional Cervical Flexion Test
Anatomy and Biomechanical Considerations:
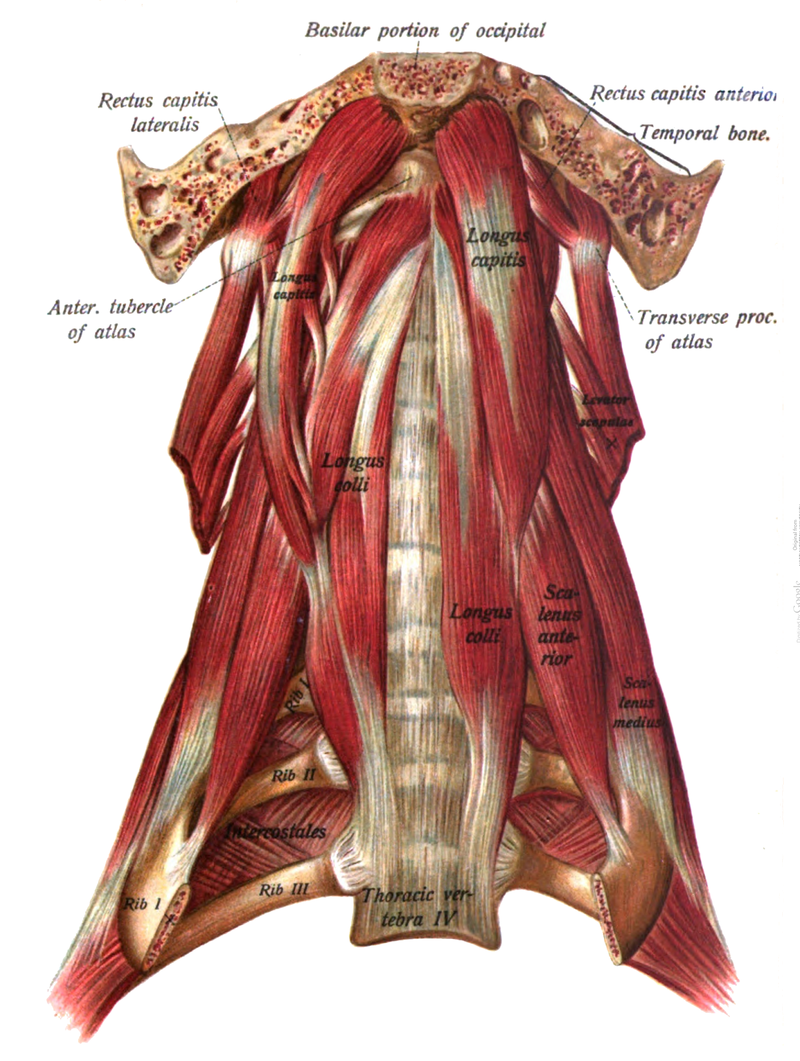
The cervical flexion test assesses the ability of the patient to segmentally flex the cervical spine using the longus colli, longus capitis and rectus capitis anterior assisted by the SCMs, anterior scalenes and infra and suprahyoid muscles. When the primary deep neck flexors are inhibited/weak the SCMs and anterior scalenes substitute for this weakness and become the primary neck flexors resulting in the chin tipping up and the upper CS extending rather than flexing during the performance of this test (Janda, 1994).
Abnormal afferent information that can contribute to this muscle imbalance can occur when ERS dysfunctions of the cervical and especially upper thoracic spine are present. These ERS dysfunctions can result in inhibition of the longus colli and longus capitis due to restricted active and passive ROM for neck flexion. In addition, hypertonicity of the scalenes occurs in apical chest wall breathers as the scalenes, which are normally only accessory muscles recruited with deep inhalation, become recruited with every breath. Palpation of the scalenes in these patients will confirm the recruitment of these muscles even during relaxed breathing. This typically is felt to occur more on the R side than the L. Asking these patients to take a deep breath while the therapist palpates the lower lateral rib cage for normal bucket handle motion will reveal restricted excursion on the R side in these patients.