Dysfunctional Hip Abduction and ER and/or Dysfunctional Hip Abduction Functional Movement Tests
These dysfunctional movement tests are best addressed by mobilizing the inferiomedial hip capsule, stretching the hip adductors and/or obturator nerve, and mobilizing the sacral base to restore restricted anterior nutation on the dysfunctional test side before retraining is initiated. Also a pubic symphysis dysfunction needs to be addressed, if present, as it represents an imbalance in tone between the hip adductors and abdominals and can contribute to, or be the source of these dysfunctional movement tests.
Mobilizing the hip in an inferiomedial direction in side lying at 45 degrees of passive hip abduction has been shown to improve isometric torque in the hip abductors, in the short term, in healthy subjects. (Makofsky et al., 2007). This response is proposed to be due to a reduction of an inhibitory and dysfunctional arthrokinetic reflex from a tight inferiomedial joint capsule (Warmerdam, 1999).
Anatomy and Biomechanical Considerations:
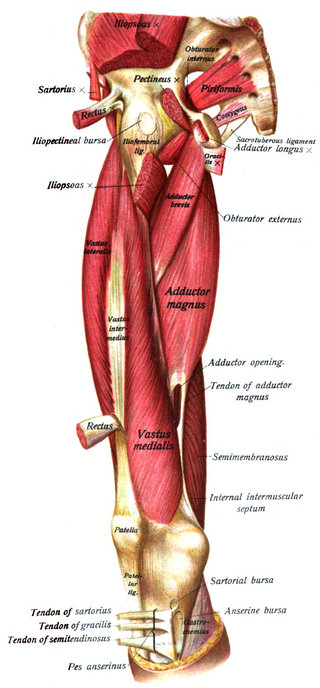
Hip Adductors
- Attach to the pubic ramus and ischial ramus to ischial tuberosity
- Function to restrain abduction of the stance limb during gait
- They also assist in internal rotation and flexion of the hip
- Hypertonicity of the hip adductors can result in displacement of the femoral head superiorly and laterally
- Innervation – obturator n. L2, 3 and 4
Anterior Oblique Sling
- Adductors are functionally connected to the abdominal obliques on the contralateral slide to form an oblique sling of support for the anterior pelvis
- When hypertonic the pull of the adductors can result in an inferior pubic shear