Dysfunctional Trunk Rotation Test
Anatomy and Biomechanics:
Active trunk rotation occurs by the combined activation of the abdominal obliques, multifidi and the erector spinae muscles. This functional movement test also requires that the patient has normal and symmetrical facet joint mobility for flexion and rotation in the lower thoracic and lumbar spines. Restricted spinal rotation, secondary to non-neutral segmental dysfunctions, especially an ERS dysfunction from T6 to L2 that limits segmental flexion and rotation, can interfere with the performance of this test. Consequently ERS dysfunctions found from T6 to L2 need to be addressed as described in module #3. before attempting to retrain this dysfunctional movement pattern with the following exercise.
Abdominal Obliques: Key Global Mobilizers for rotation of the thoracic and lumbar spine and pelvis.
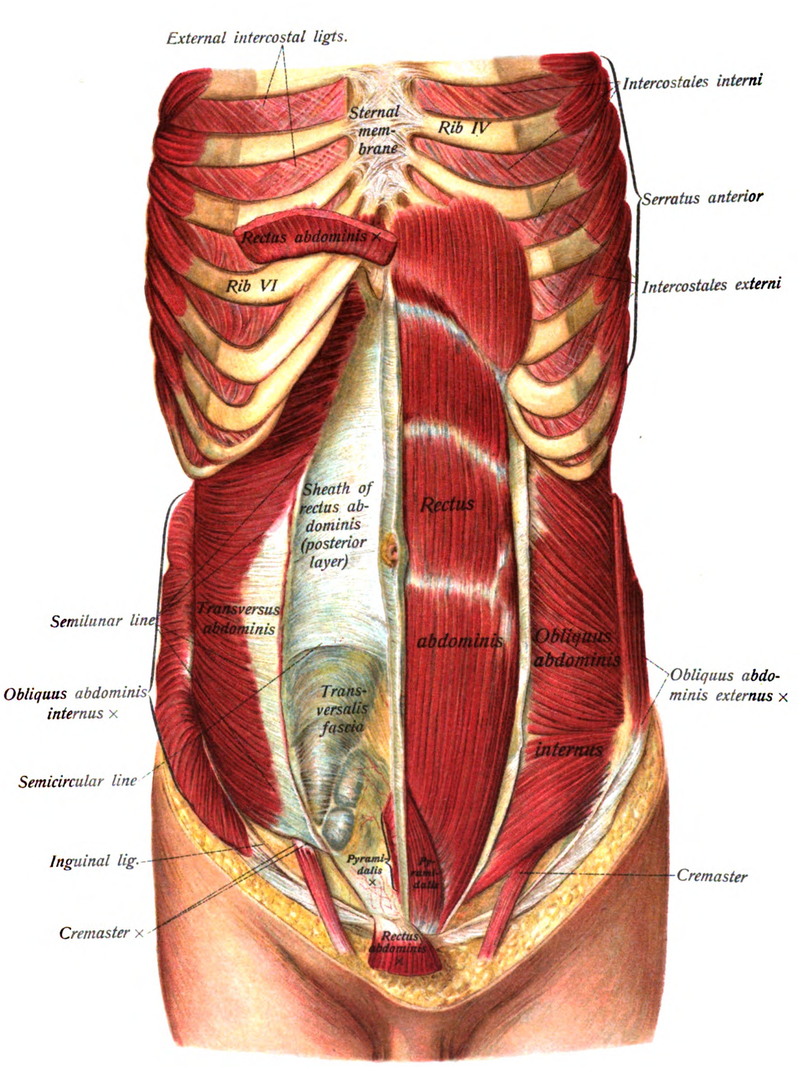
External Obliques – Anterior fibers attach from ribs 5 thru 8 and interdigitate with the serratus anterior. They insert into the linea alba through a broad flat aponeurosis. The lateral fibers attach from ribs 9 thru 12 and interdigitate with the latissimus dorsi. They form the inguinal ligament running from the ASIS to the pubic tubercle. Acting bilaterally they flex the lumbar spine and posteriorly tilt the pelvis. Acting unilaterally they laterally flex the spine to the same side and rotate away, similar to the action of the SCMs.
Innervation – T5 to T12 intercostal nerves
Internal Obliques – Anterior fibers attach along the lateral two-thirds of the inguinal ligament and iliac crest and insert into the crest of the pubis and linea alba. The lateral fibers attach to the middle third of the iliac crest and thoracolumbar fascia and insert to the inferior borders of ribs 10-12. Acting bilaterally they flex and posteriorly rotate the pelvis. Acting unilaterally with the anterior fibers of the external obliques on the opposite side they rotate the thorax forward, when the pelvis is fixed, or rotate the pelvis backward when the thorax is fixed.
Innervation – T7-12 intercostal nerves, iliohypogastric and ilioinguinal nerves
The oblique abdominals also have a vertical component to their orientation meaning that when they contract they also cause simultaneous flexion of the trunk and therefore the lumbar spine. The role of the multifidus in rotation is to oppose this flexion effect and not by themselves do they produce rotation of the spine (Bogduk and Twomey, 1991).
Substitution Patterns to watch out for during retraining:
Patients will often substitute by using the hip external rotators to bring the legs and pelvis back to the table rather than using the obliques when performing this test. Therefore the therapist should instruct the patient to initiate and perform this movement from the trunk and not from the hips. We propose that hypertonicity and chronic tightness of the hip external rotators, especially the piriformis, may be due to this dysfunctional motor control substitution pattern.
Patients will often substitute by overutilization not only of the hip external rotators, but also by using the quadratus lumborum or the lateral fibers of the obliques resulting in frontal plane side bending. They may also substitute for the multifidus by using the erector spinae muscles resulting in excessive segmental extension to compensate for the lack of control in the transverse plane. Therefore the therapist should watch for any trunk side bending or spinal extension that may occur when retraining the patient in the performance of the following exercise. Not only can these substitution patterns be palpated with your fingers placed alongside the spinous processes as demonstrated in module #2, but an astute therapist can often observe these substitution patterns as they occur by asking the patient to slowly and repeatedly rotate the legs and pelvis back and forth from side to side.